

Performance of HIV-1 drug resistance testing at low-level viremia and its ability to predict future virologic outcomes and viral evolution in treatment-naive individuals
- PMID: 24429436
- PMCID: PMC3967823
- DOI: 10.1093/cid/ciu019
Performance of HIV-1 drug resistance testing at low-level viremia and its ability to predict future virologic outcomes and viral evolution in treatment-naive individuals
Abstract
Background: Low-level viremia (LLV; human immunodeficiency virus [HIV-1] RNA 50-999 copies/mL) occurs frequently in patients receiving antiretroviral therapy (ART), but there are few or no data available demonstrating that HIV-1 drug resistance testing at a plasma viral load (pVL) <1000 copies/mL provides potentially clinically useful information. Here, we assess the ability to perform resistance testing by genotyping at LLV and whether it is predictive of future virologic outcomes in patients beginning ART.
Methods: Resistance testing by genotyping at LLV was attempted on 4915 plasma samples from 2492 patients. A subset of previously ART-naive patients was analyzed who achieved undetectable pVL and subsequently rebounded with LLV (n = 212). A genotypic sensitivity score (GSS) was calculated based on therapy and resistance testing results by genotyping, and stratified according to number of active drugs.
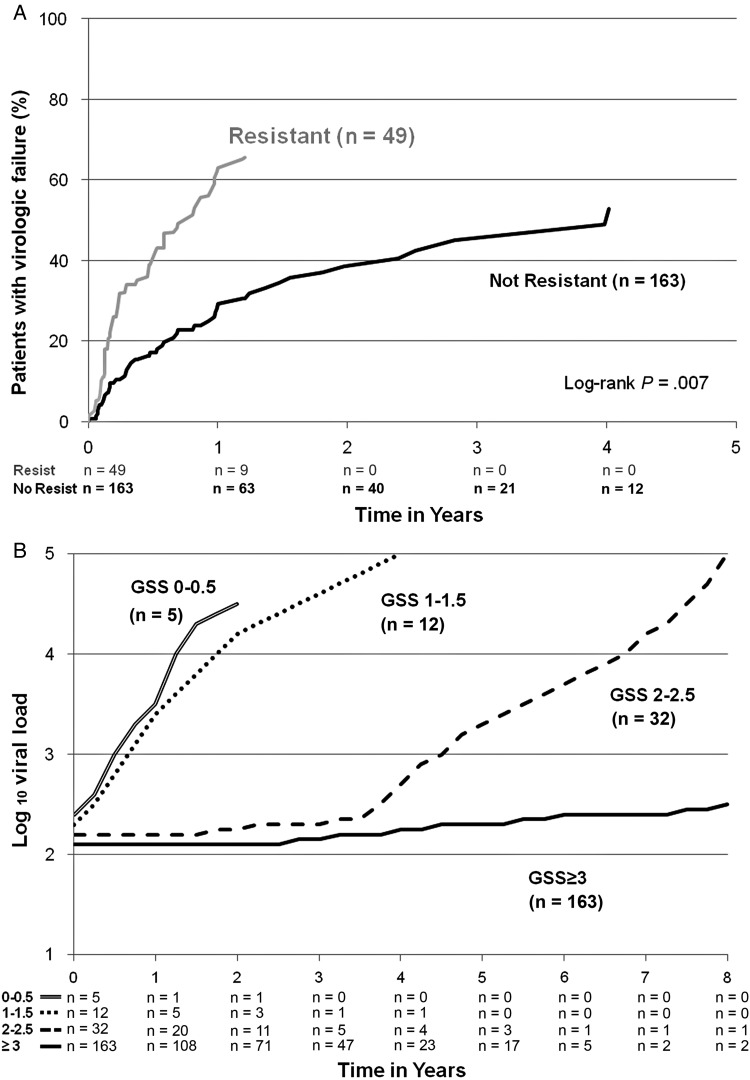
Results: Eighty-eight percent of LLV resistance assays produced useable sequences, with higher success at higher pVL. Overall, 16 of 212 (8%) patients had pretherapy resistance. Thirty-eight of 196 (19%) patients without pretherapy resistance evolved resistance to 1 or more drug classes, primarily the nucleoside reverse transcriptase (14%) and/or nonnucleoside reverse transcriptase (9%) inhibitors. Patients with resistance at LLV (GSS <3) had a 2.1-fold higher risk of virologic failure (95% confidence interval, 1.2- to 3.7-fold) than those without resistance (P = .007). Progressively lower GSS scores at LLV were associated with a higher increase in pVL over time (P < .001). Acquisition of additional resistance mutations to a new class of antiretroviral drugs during LLV was not found in a subset of patients.
Conclusions: Routine HIV-1 genotyping of LLV samples can be performed with a reasonably high success rate, and the results appear predictive of future virologic outcomes.
Keywords: ART; HIV-1; low-level viremia; outcome; resistance.
Figures


Comment in
-
Editorial Commentary: Extending HIV drug resistance testing to low levels of plasma viremia.Clin Infect Dis. 2014 Apr;58(8):1174-5. doi: 10.1093/cid/ciu025. Epub 2014 Jan 14. Clin Infect Dis. 2014. PMID: 24429434 No abstract available.
References
-
- Bansi L, Sabin C, Delpech V, et al. Trends over calendar time in antiretroviral treatment success and failure in HIV-1 clinic populations. HIV-1 Med. 2010;11:432–8. - PubMed
-
- Cohen C. Low-level viremia in HIV-1 infection: consequences and implications for switching to a new regimen. HIV-1 Clin Trials. 2009;10:116–24. - PubMed
-
- Karlsson AC, Younger SR, Martin JN, et al. Immunologic and virologic evolution during periods of intermittent and persistent low-level viremia. AIDS. 2004;18:981–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
