

Noninvasive detection of response and resistance in EGFR-mutant lung cancer using quantitative next-generation genotyping of cell-free plasma DNA
- PMID: 24429876
- PMCID: PMC3959249
- DOI: 10.1158/1078-0432.CCR-13-2482
Noninvasive detection of response and resistance in EGFR-mutant lung cancer using quantitative next-generation genotyping of cell-free plasma DNA
Abstract
Purpose: Tumor genotyping using cell-free plasma DNA (cfDNA) has the potential to allow noninvasive assessment of tumor biology, yet many existing assays are cumbersome and vulnerable to false-positive results. We sought to determine whether droplet digital PCR (ddPCR) of cfDNA would allow highly specific and quantitative assessment of tumor genotype.
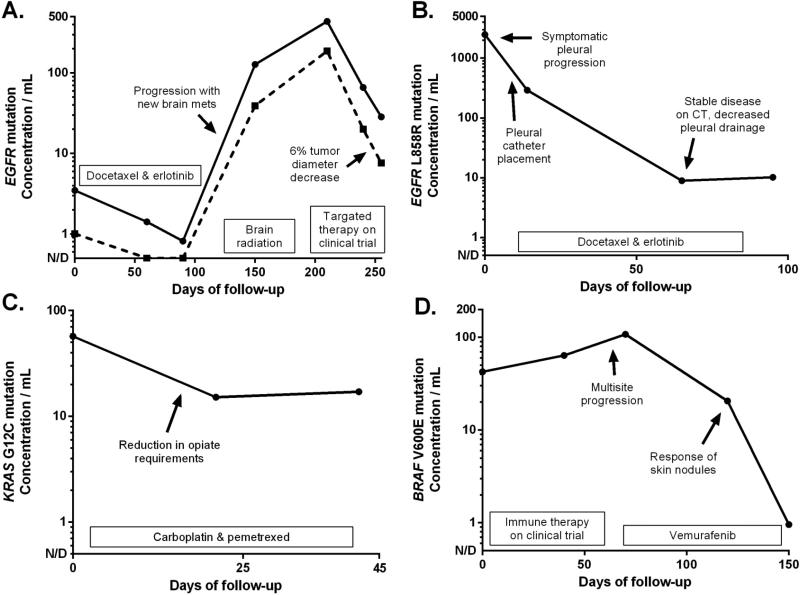
Experimental design: ddPCR assays for EGFR, KRAS, and BRAF mutations were developed using plasma collected from patients with advanced lung cancer or melanoma of a known tumor genotype. Sensitivity and specificity were determined using cancers with nonoverlapping genotypes as positive and negative controls. Serial assessment of response and resistance was studied in patients with EGFR-mutant lung cancer on a prospective trial of erlotinib.
Results: We identified a reference range for EGFR L858R and exon 19 deletions in specimens from KRAS-mutant lung cancer, allowing identification of candidate thresholds with high sensitivity and 100% specificity. Received operative characteristic curve analysis of four assays demonstrated an area under the curve in the range of 0.80 to 0.94. Sensitivity improved in specimens with optimal cfDNA concentrations. Serial plasma genotyping of EGFR-mutant lung cancer on erlotinib demonstrated pretreatment detection of EGFR mutations, complete plasma response in most cases, and increasing levels of EGFR T790M emerging before objective progression.
Conclusions: Noninvasive genotyping of cfDNA using ddPCR demonstrates assay qualities that could allow effective translation into a clinical diagnostic. Serial quantification of plasma genotype allows noninvasive assessment of response and resistance, including detection of resistance mutations up to 16 weeks before radiographic progression.
©2014 AACR.
Figures




References
-
- Paez JG, Janne PA, Lee JC, Tracy S, Greulich H, Gabriel S, et al. EGFR Mutations in Lung Cancer: Correlation with Clinical Response to Gefitinib Therapy. Science. 2004;304:1497–500. - PubMed
-
- Karapetis CS, Khambata-Ford S, Jonker DJ, O'Callaghan CJ, Tu D, Tebbutt NC, et al. K-ras Mutations and Benefit from Cetuximab in Advanced Colorectal Cancer. N Engl J Med. 2008;359:1757–65. - PubMed
-
- Jackman DM, Miller VA, Cioffredi LA, Yeap BY, Janne PA, Riely GJ, et al. Impact of epidermal growth factor receptor and KRAS mutations on clinical outcomes in previously untreated non-small cell lung cancer patients: results of an online tumor registry of clinical trials. Clin Cancer Res. 2009;15:5267–73. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
