

Apparent and true resistant hypertension: definition, prevalence and outcomes
- PMID: 24430707
- PMCID: PMC4090282
- DOI: 10.1038/jhh.2013.140
Apparent and true resistant hypertension: definition, prevalence and outcomes
Abstract
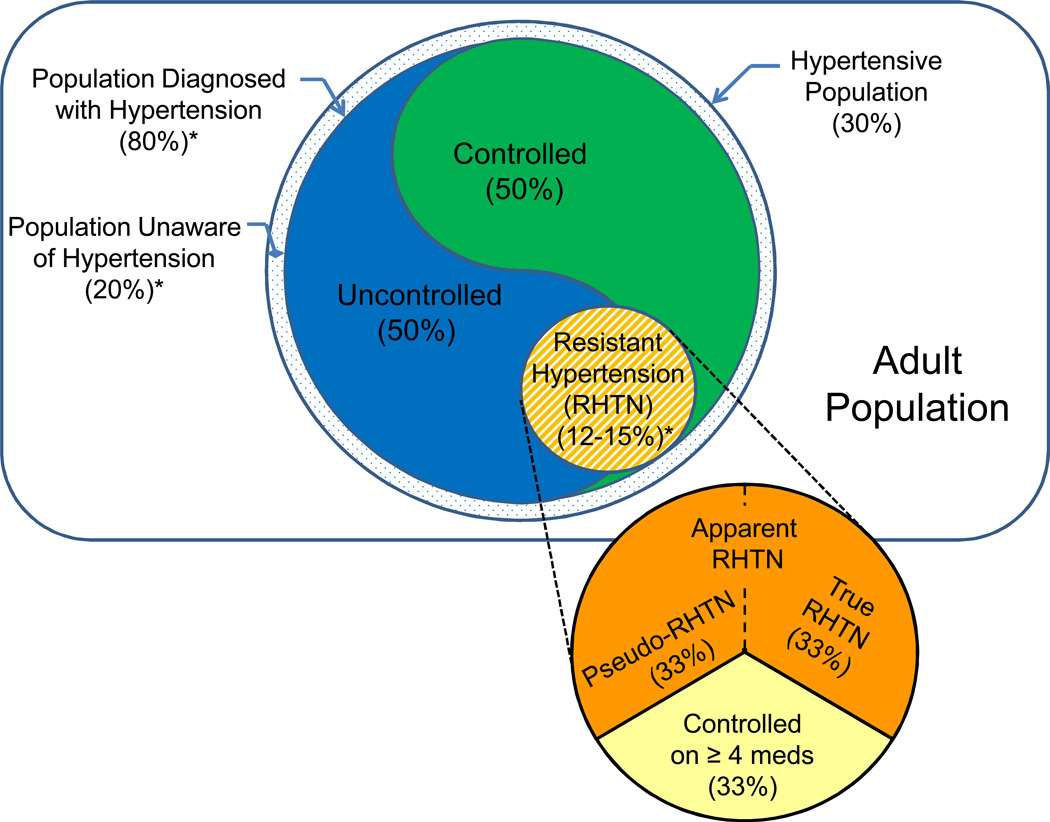
Resistant hypertension, defined as blood pressure (BP) remaining above goal despite the use of > or =3 antihypertensive medications at maximally tolerated doses (one ideally being a diuretic) or BP that requires > or =4 agents to achieve control, has received more attention with increased efforts to improve BP control rates and the emergence of device-based therapies for hypertension. This classically defined resistant group consists of patients with true resistant hypertension, controlled resistant hypertension and pseudo-resistant hypertension. In studies where pseudo-resistant hypertension cannot be excluded (for example, 24-h ambulatory BP not obtained), the term apparent resistant hypertension has been used to identify 'apparent' lack of control on > or =3 medications. Large, well-designed studies have recently reported the prevalence of resistant hypertension. Pooling prevalence data from these studies and others within North America and Europe with a combined sample size of >600,000 hypertensive participants, the prevalence of resistant hypertension is 14.8% of treated hypertensive patients and 12.5% of all hypertensives. However, the prevalence of true resistant hypertension, defined as uncontrolled both by office and 24-h ambulatory BP monitoring with confirmed medication adherence, may be more meaningful in terms of identifying risk and estimating benefit from newer therapies like renal denervation. Rates of cardiovascular events and mortality follow mean 24-h ambulatory BPs in patients with resistant hypertension, and true resistant hypertension represents the highest risk. The prevalence of true resistant hypertension has not been directly measured in large trials; however, combined data from smaller studies suggest that true resistant hypertension is present in half of the patients with resistant hypertension who are uncontrolled in the office. Our pooled analysis shows prevalence rates of 10.1% and 7.9% for uncontrolled resistant hypertension among individuals treated for hypertension and all hypertensive individuals, respectively.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Kearney PM, Whelton M, Reynolds K, Whelton PK, He J. Worldwide prevalence of hypertension: a systematic review. J Hypertens. 2004;22:11–19. - PubMed
-
- Wolf-Maier K, Cooper RS, Banegas JR, Giampaoli S, Hense HW, Joffres M, et al. Hypertension and blood pressure levels in 6 European countries, Canada, and the US. JAMA. 2003;289:2363–2369. - PubMed
-
- Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988–2008. JAMA. 2010;303:2043–2050. - PubMed
-
- Falaschetti E, Chaudhury M, Mindell J, Poulter N. Continued improvement in hypertension management in England: results from the Health Survey for England 2006. Hypertension. 2009;53:480–486. - PubMed
-
- Verdecchia P, Gentile G, Angeli F, Mazzotta G, Mancia G, Reboldi G. Influence of blood pressure reduction on composite cardiovascular endpoints in clinical trials. J Hypertens. 2010;28:1356–1365. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
