

Pediatric tracheotomy: indications and decannulation outcomes
- PMID: 24430892
- PMCID: PMC4099419
- DOI: 10.1002/lary.24596
Pediatric tracheotomy: indications and decannulation outcomes
Abstract
Objectives/hypothesis: The objective of this study was to determine if there are differences in decannulation rates and duration of cannulation between pediatric patients undergoing tracheotomy for different indications.
Study design: Retrospective chart review.
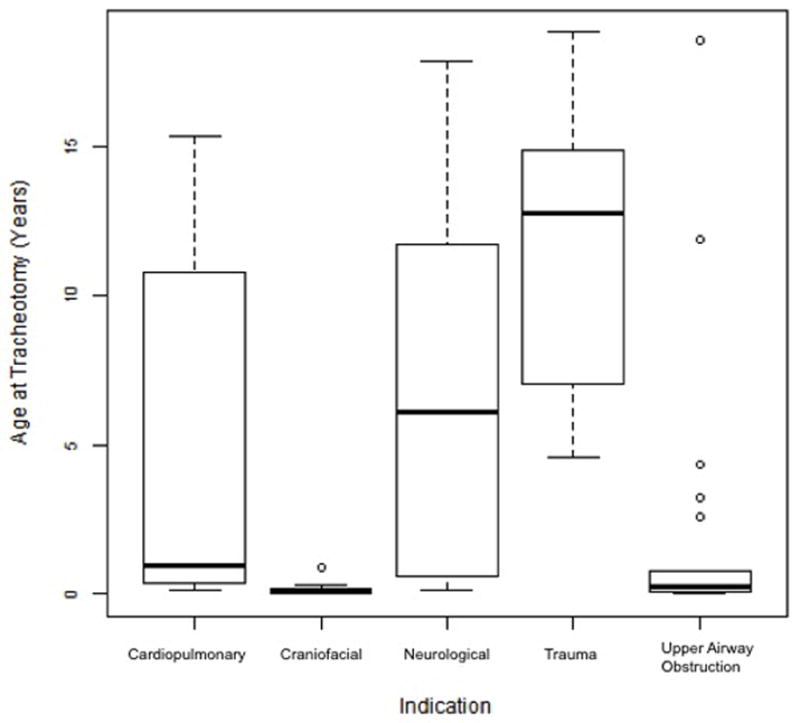
Methods: Medical records for pediatric patients (age 0-18 years) undergoing tracheotomy between January 1, 2003, and May 31, 2012, were retrospectively reviewed. Patients were assigned an indication for tracheotomy from five categories: neurological, cardiopulmonary, upper airway obstruction, craniofacial anomalies, and maxillofacial/laryngotracheal trauma.
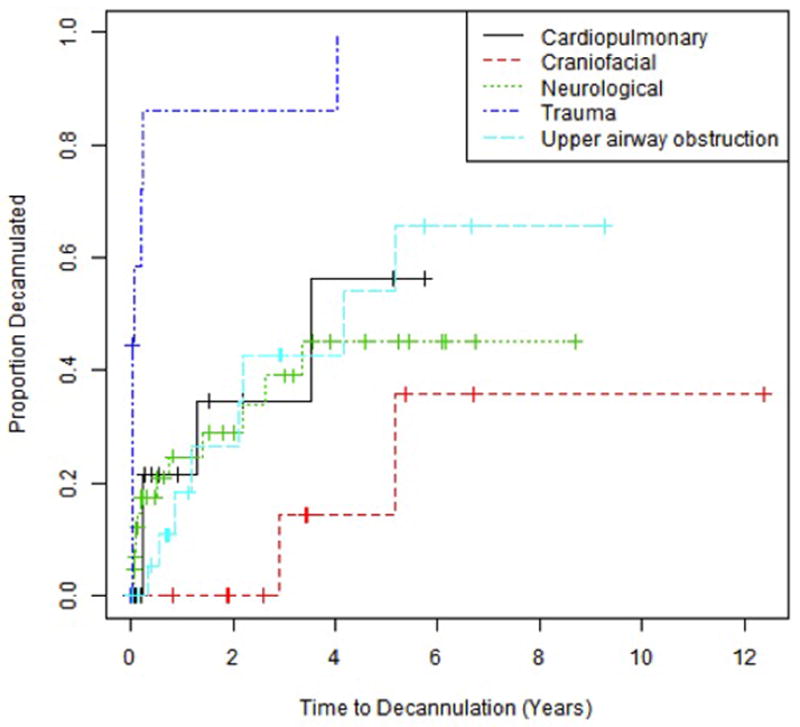
Results: Initial chart review identified 124 patients, 113 for whom complete data was available. Of these patients, the indications for tracheotomy were cardiopulmonary disease in 24 (21.2%), craniofacial anomalies in 12 (10.6%), neurological impairment in 44 (38.9%), traumatic injury in 11 (9.7%), and upper airway obstruction in 22 (19.5%). The time to decannulation was shorter for trauma patients compared to cardiopulmonary (P = 0.044) and neurological patients (P = 0.001). A total of 32 (31.9%) patients were decannulated during the study period, with a higher rate in trauma patients (72.7%) and a lower rate in those with upper airway obstruction (36.4%) than would be expected under homogeneity. Of the 32 patients who were decannulated, 11 (30.6%) were decannulated during the same hospitalization in which the tracheotomy was performed.
Conclusion: This study demonstrates a difference in overall decannulation rates and a shorter time to decannulation in children undergoing tracheotomy for maxillofacial and laryngotracheal trauma compared to cardiopulmonary and neurological indications.
Keywords: Pediatric tracheotomy; decannulation; tracheostomy; upper airway obstruction.
© 2014 The American Laryngological, Rhinological and Otological Society, Inc.
Conflict of interest statement
Figures
References
-
- Lewis CW, Carron JD, Perkins JA, Sie KC, Feudtner C. Tracheotomy in pediatric patients: a national perspective. Arch Otolaryngol Head Neck Surg. 2003;129:523–529. - PubMed
-
- Hadfield PJ, Lloyd-Faulconbridge RV, Almeyda J, Albert DM, Bailey CM. The changing indications for paediatric tracheostomy. Int J Pediatr Otorhinolaryngol. 2003;67:7. - PubMed
-
- Carron JD, Derkay CS, Strope GL, Nosonchuk JE, Darrow DH. Pediatric tracheotomies: changing indications and outcomes. Laryngoscope. 2000;110:1099–1104. - PubMed
-
- Line WS, Jr, Hawkins DB, Kahlstrom EJ, MacLaughlin EF, Ensley JL. Tracheotomy in infants and young children: the changing perspective 1970–1985. Laryngoscope. 1986;96:510–515. - PubMed
-
- Dursun O, Ozel D. Early and long-term outcome after tracheostomy in children. Pediatr Int. 2001;53:202–206. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
