

Overview of foot deformity management in children with cerebral palsy
- PMID: 24432097
- PMCID: PMC3838514
- DOI: 10.1007/s11832-013-0509-4
Overview of foot deformity management in children with cerebral palsy
Abstract
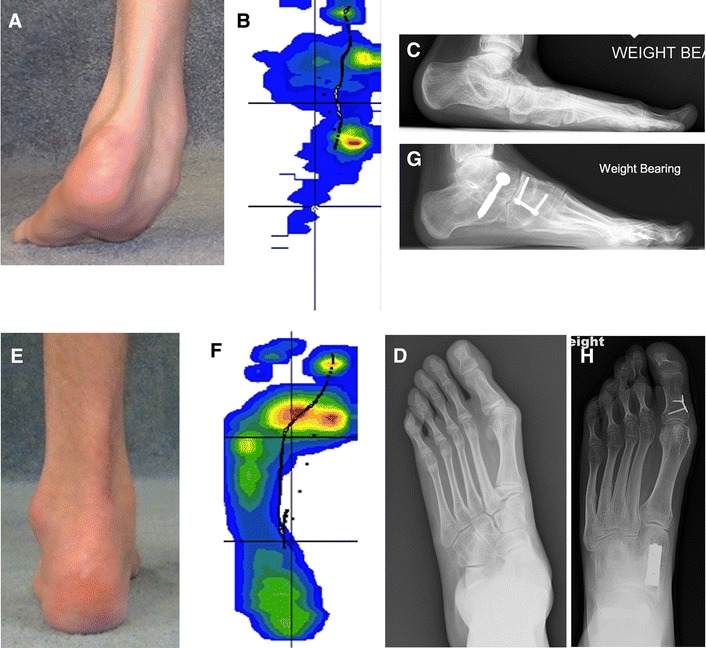
Foot deformities in children with cerebral palsy are common. The natural history of the deformities of the feet is very variable and very unpredictable in young children less then 5 years old. Treatment for the young children should be primarily with orthotics and manual therapy. Equinus is the most common deformity, with orthotics augmented with botulinum toxin being the primary management in young children. When fixed deformity develops lengthening only the muscle which is contracted is preferred. Varus deformity of the feet is often associated with equinus, and can almost always be managed with orthotics until 8 or 10 years of age. Planovalgus is the most common deformity in children with bilateral lower extremity spasticity. The primary management is orthotics until the child no longer tolerates the orthotic; then surgical management needs to consider all the deformities and all should be corrected. This requires correcting the subtalor subluxation with calcaneal lengthening or fusion, medial midfoot correction with osteotomy or fusion.
Keywords: Cerebral palsy; Equinovarus; Equinus; Planovalgus feet.
Figures
References
-
- Wren TA, Cheatwood AP, Rethlefsen SA, Hara R, Perez FJ, Kay RM. Achilles tendon length and medial gastrocnemius architecture in children with cerebral palsy and equinus gait. JPO. 2012;30:479–484. - PubMed
-
- Dreher R, Buccoliero T, Wolf SI, Heitzmann D, Gantz S, Braatz F, Wenz W (2012) Long-term results after gastrocnemius–soleus intramuscular aponeurotic recession as a part of multilevel surgery in spastic diplegic cerebral palsy. JBJS 94:627–637 - PubMed
-
- Svehlik M, Kraus T, Steinwender G, Zwick EB, Saraph V, Linhart WE. The Baumann procedure to correct equinus gait in children with diplegic cerebral palsy: long-term results. JBJS. 2012;94:1143–1147. - PubMed
-
- Davids JR, Rogozinski BM, Hardin JW, Davis RB (2011) Ankle dorsiflexor function after plantar flexor surgery in children with cerebral palsy. JBJS 93:e1381–1387 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
