

Longitudinal epiphyseal bracket
- PMID: 24432108
- PMCID: PMC3886355
- DOI: 10.1007/s11832-013-0544-1
Longitudinal epiphyseal bracket
Abstract
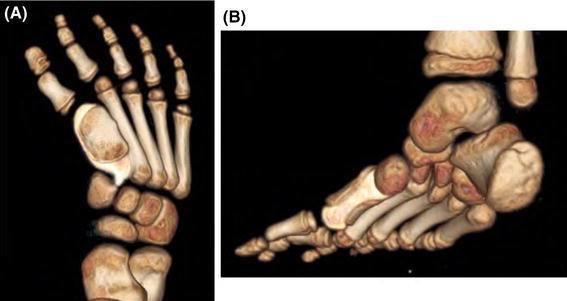
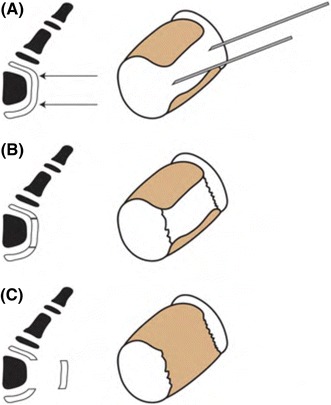
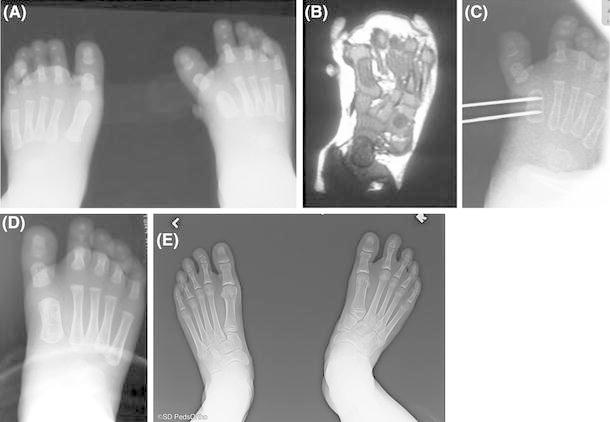
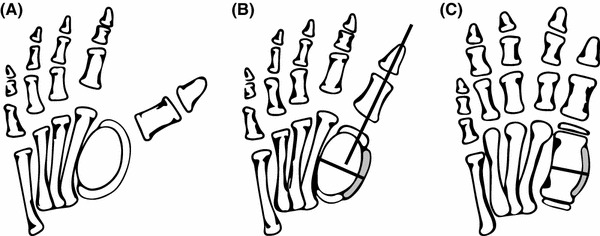
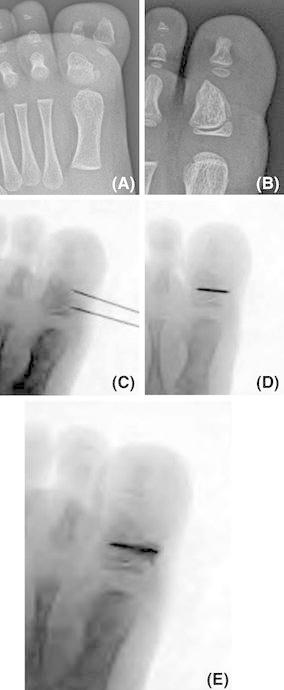
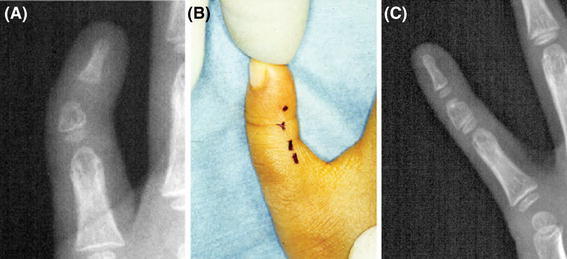
Longitudinal epiphyseal bracket or bracket epiphysis is an uncommon disorder of growth. Alternatively known as a delta phalanx, it is due to an anomalous secondary ossification center that extends longitudinally along the diaphysis. Although rare, longitudinal epiphyseal bracket most commonly manifests in the hands as clinodactyly and in the feet as hallux varus. Previously, longitudinal epiphyseal bracket has been treated with angular osteotomy, but we recommend early surgical physiolysis. We describe this uncommon disorder, our current recommendation for treatment, and present three illustrative cases.
Keywords: Bracket epiphysis; Clinodactyly; Delta phalanx; Hallux varus; Longitudinal epiphyseal bracket; Physiolysis.
Figures


References
-
- Jones GB. Delta phalanx. J Bone Joint Surg Br. 1964;46:226–228. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
