

Complications of muscle injuries
- PMID: 24432177
- PMCID: PMC3846951
- DOI: 10.1007/s40477-013-0010-4
Complications of muscle injuries
Abstract
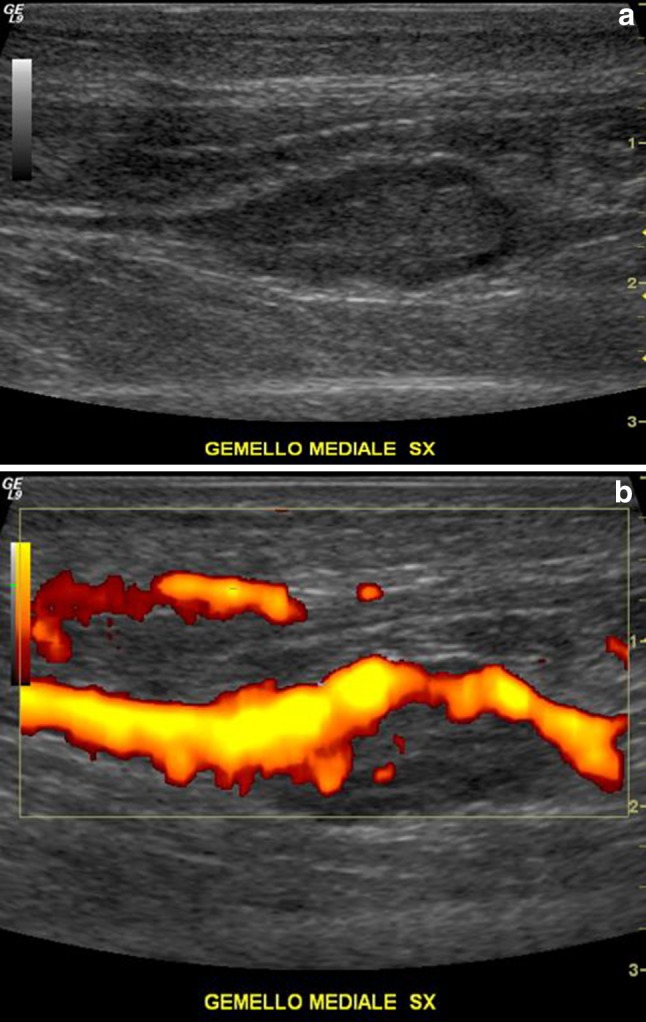
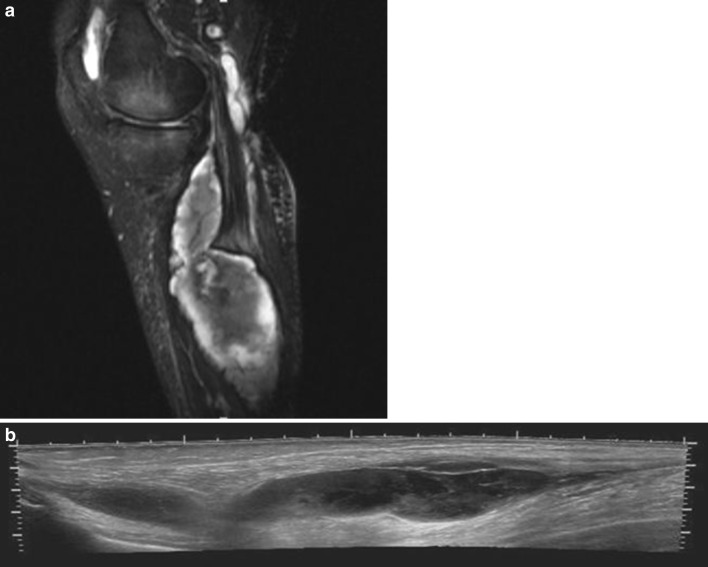
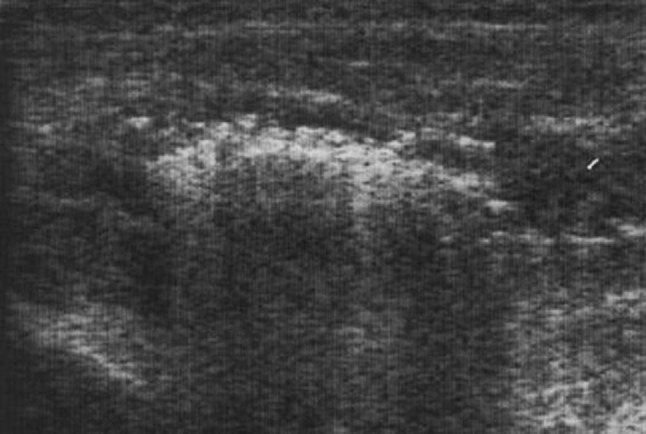
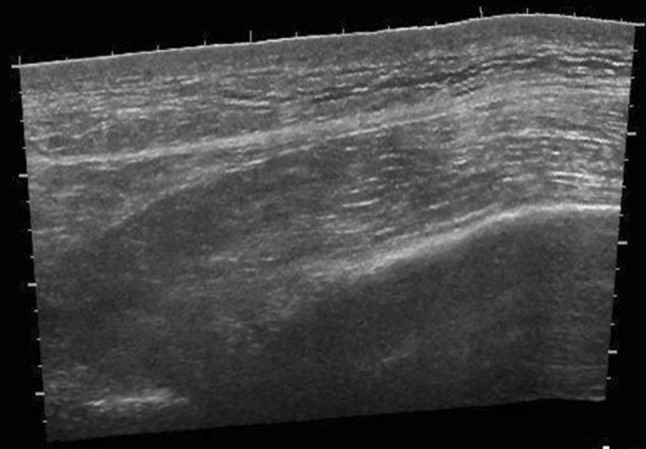
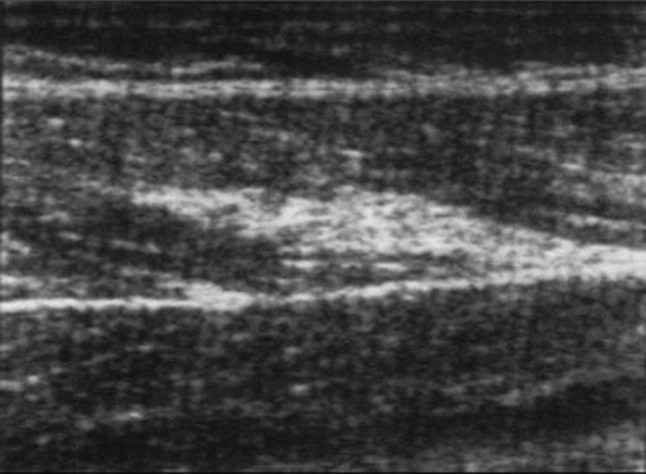
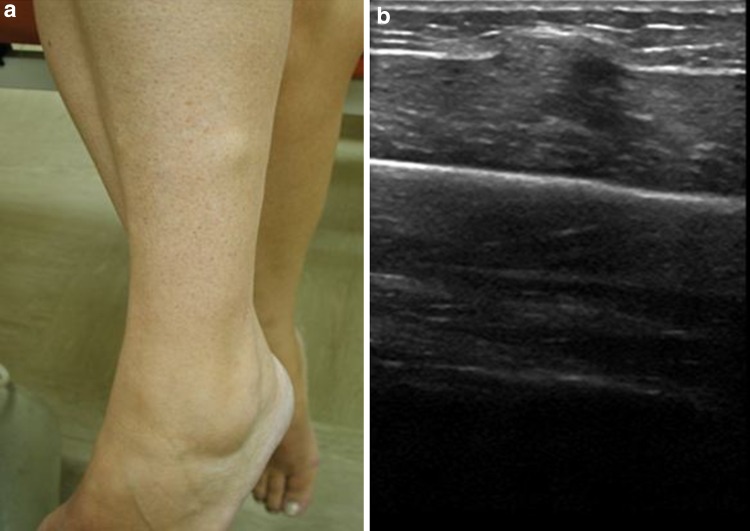
Muscle injuries can be classified into strain injuries and contusions. Depending on the type of injury, different complications may occur, which in turn can be divided into early, intermediate and delayed complications. A prompt diagnosis of complications allows early treatment and permits to avoid harmful sequelae. Imaging studies, ultrasonography in particular, allow (recognizing) the assessment of complications whenever clinically suspected. In this article the most frequent complications of muscle injuries are presented.
Le lesioni muscolari possono essere classificate in lesioni contusive e lesioni distrattive. A seconda del tipo di lesione, possono insorgere complicanze differenti, che a loro volta possono essere suddivise in complicanze precoci, intermedie e tardive. Un rapido e preciso riconoscimento delle complicanze consente di intervenire precocemente e permette di evitare conseguenze dannose. L’imaging, in particolar modo l’ecografia, permette il riconoscimento di complicanze ogni qualvolta esse siano sospettate clinicamente. In questo articolo vengono presentate le complicanze più frequenti delle lesioni muscolari.
Keywords: Complications; Muscle injuries; Ultrasound.
Figures
References
-
- Bianchi S, Martinoli C, Abdelwahab IF, Derchi LE, Damiani S. Sonographic evaluation of tears of the gastrocnemius medial head (“tennis leg”) J Ultrasound Med. 1998;17(3):157–162. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
