

Review of ultrasonography of malignant neck nodes: greyscale, Doppler, contrast enhancement and elastography
- PMID: 24434158
- PMCID: PMC3894696
- DOI: 10.1102/1470-7330.2013.0056
Review of ultrasonography of malignant neck nodes: greyscale, Doppler, contrast enhancement and elastography
Abstract
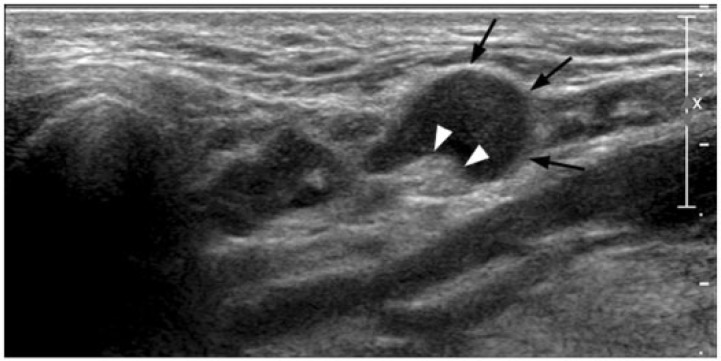
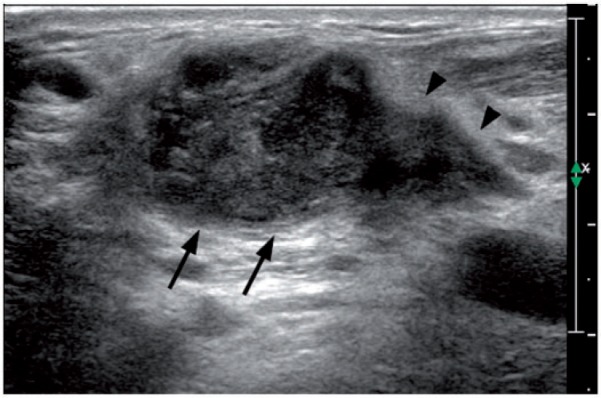
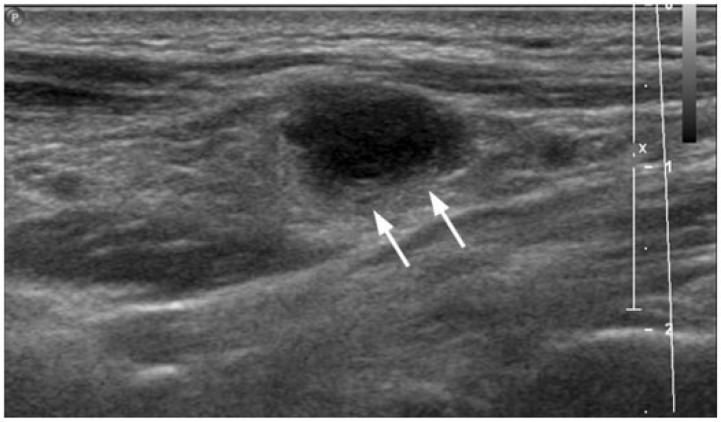
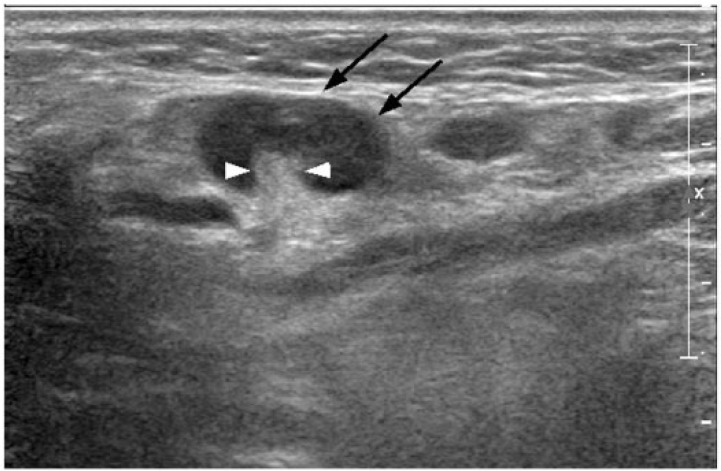
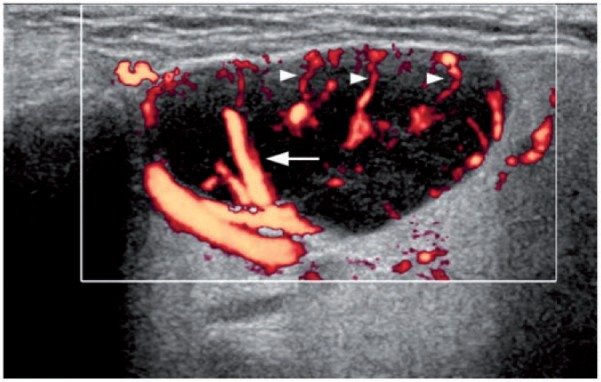
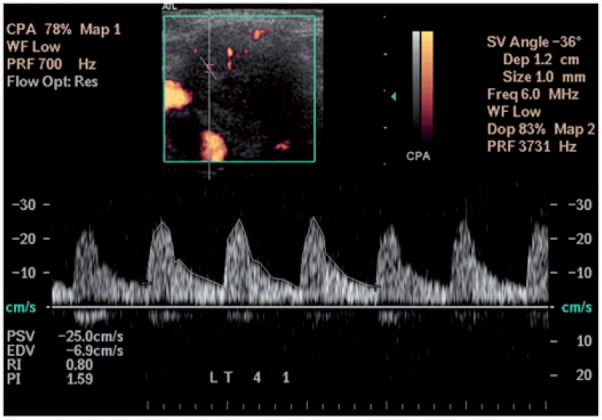
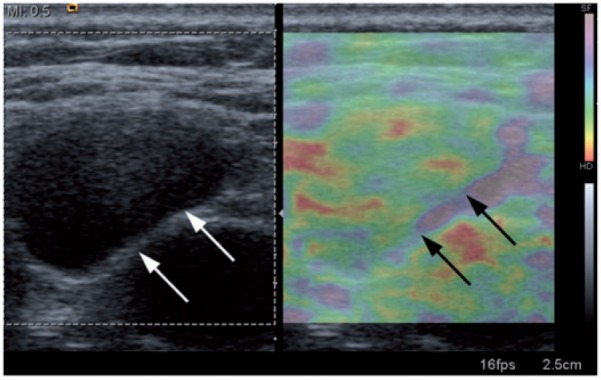
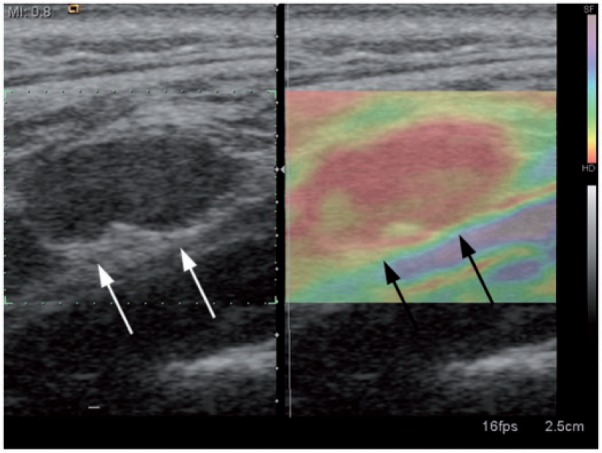
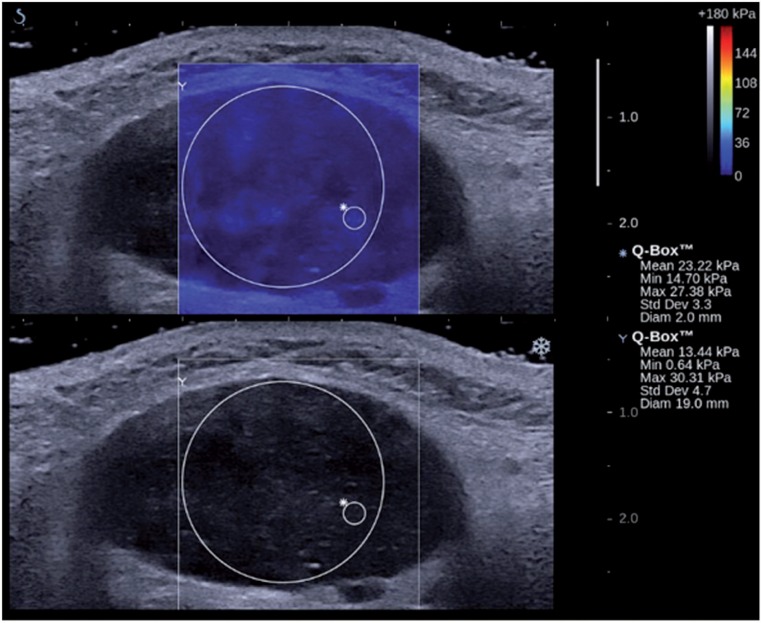
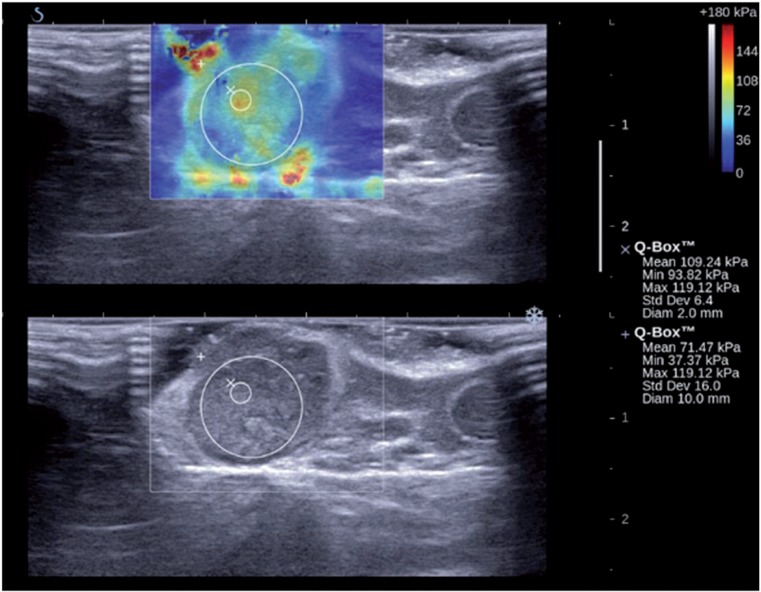
Assessment of neck lymph nodes is essential in patients with head and neck cancers for predicting the patient's prognosis and selecting the appropriate treatment. Ultrasonography is a useful imaging tool in the assessment of neck lymph nodes. Greyscale ultrasonography assesses the size, distribution, and internal architecture of lymph nodes. Doppler ultrasonography evaluates the intranodal vascular pattern and resistance of lymph nodes. Contrast-enhanced ultrasonography provides information on lymph node parenchymal perfusion. Elastography allows qualitative and quantitative assessment of lymph node stiffness. This article reviews the value of greyscale, Doppler and contrast-enhanced ultrasonography as well as elastography in the assessment of malignant nodes in the neck.
Figures

Similar articles
-
Sonography of neck lymph nodes. Part II: abnormal lymph nodes.Clin Radiol. 2003 May;58(5):359-66. doi: 10.1016/s0009-9260(02)00585-8. Clin Radiol. 2003. PMID: 12727163 Review.
-
Shear Wave Elastography in Head and Neck Lymph Node Assessment: Image Quality and Diagnostic Impact Compared with B-Mode and Doppler Ultrasonography.Ultrasound Med Biol. 2016 Feb;42(2):387-98. doi: 10.1016/j.ultrasmedbio.2015.10.019. Epub 2015 Nov 23. Ultrasound Med Biol. 2016. PMID: 26617244
-
Ultrasound of malignant cervical lymph nodes.Cancer Imaging. 2008 Mar 25;8(1):48-56. doi: 10.1102/1470-7330.2008.0006. Cancer Imaging. 2008. PMID: 18390388 Free PMC article. Review.
-
[Introduction to ultrasonography of lymph nodes of the neck].Ugeskr Laeger. 2009 Feb 2;171(6):423-6. Ugeskr Laeger. 2009. PMID: 19208332 Danish.
-
Real-time ultrasound elastography: an assessment of enlarged cervical lymph nodes.Eur Radiol. 2013 Sep;23(9):2351-7. doi: 10.1007/s00330-013-2861-7. Epub 2013 May 8. Eur Radiol. 2013. PMID: 23652848
Cited by
-
Quantification of intranodal vascularity by computer pixel-counting method enhances the accuracy of ultrasound in distinguishing metastatic and tuberculous cervical lymph nodes.Quant Imaging Med Surg. 2019 Nov;9(11):1773-1780. doi: 10.21037/qims.2019.10.02. Quant Imaging Med Surg. 2019. PMID: 31867231 Free PMC article.
-
Post-pandemic healthcare for COVID-19 vaccine: Tissue-aware diagnosis of cervical lymphadenopathy via multi-modal ultrasound semantic segmentation.Appl Soft Comput. 2023 Jan;133:109947. doi: 10.1016/j.asoc.2022.109947. Epub 2022 Dec 19. Appl Soft Comput. 2023. PMID: 36570119 Free PMC article.
-
A clinical compilation of lymph node pathologies comparing the diagnostic performance of biopsy methods.J Ultrasound. 2019 Mar;22(1):59-64. doi: 10.1007/s40477-018-0321-6. Epub 2018 Oct 4. J Ultrasound. 2019. PMID: 30284690 Free PMC article.
-
Elastography Enhances the Diagnostic Performance of Conventional Ultrasonography in Differentiating Benign from Malignant Superficial Lymphadenopathies.Cancers (Basel). 2025 Apr 28;17(9):1480. doi: 10.3390/cancers17091480. Cancers (Basel). 2025. PMID: 40361407 Free PMC article.
-
Contrast-enhanced ultrasound (CEUS) in characterization of inconclusive cervical lymph nodes: a meta-analysis and systematic review.Sci Rep. 2022 May 12;12(1):7804. doi: 10.1038/s41598-022-11542-9. Sci Rep. 2022. PMID: 35551228 Free PMC article.
References
-
- Vassallo P, Wernecke K, Roos N, Peters PE. Differentiation of benign from malignant superficial lymphadenopathy: the role of high-resolution US. Radiology. 1992;183:215. PMid:1549675. - PubMed
-
- Som PM. Detection of metastasis in cervical lymph nodes: CT and MR criteria and differential diagnosis. Am J Roentgenol. 1992;158:961. - PubMed
-
- Baatenburg de Jong RJ, Rongen RJ, Lameris JS, Harthoorn M, Verwoerd CD, Knegt P. Metastatic neck disease. Palpation vs ultrasound examination. Arch Otolaryngol Head Neck Surg. 1989;115:689. PMid:2655666. - PubMed
-
- Bruneton JN, Normand F. Cervical lymph nodes. In: Bruneton JN, editor. Ultrasonography of the neck. Berlin: Springer-Verlag; 1987. p. 81.
-
- Baatenburg de Jong RJ, Rongen RJ, Verwoerd CD, van Overhagen H, Lameris JS, Knegt P. Ultrasound-guided fine-needle aspiration biopsy of neck nodes. Arch Otolaryngol Head Neck Surg. 1991;117:402. PMid:2007009. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical