

Effect of food insecurity on chronic kidney disease in lower-income Americans
- PMID: 24434743
- PMCID: PMC3952065
- DOI: 10.1159/000357595
Effect of food insecurity on chronic kidney disease in lower-income Americans
Abstract
Background: The relation of food insecurity (inability to acquire nutritionally adequate and safe foods) and chronic kidney disease (CKD) is unknown. We examined whether food insecurity is associated with prevalent CKD among lower-income individuals in both the general US adult population and an urban population.
Methods: We conducted cross-sectional analyses of lower-income participants of the National Health and Nutrition Examination Survey (NHANES) 2003-2008 (n = 9,126) and the Healthy Aging in Neighborhoods of Diversity across the Life Span (HANDLS) study (n = 1,239). Food insecurity was defined based on questionnaires and CKD was defined by reduced estimated glomerular filtration rate or albuminuria; adjustment was performed with multivariable logistic regression.
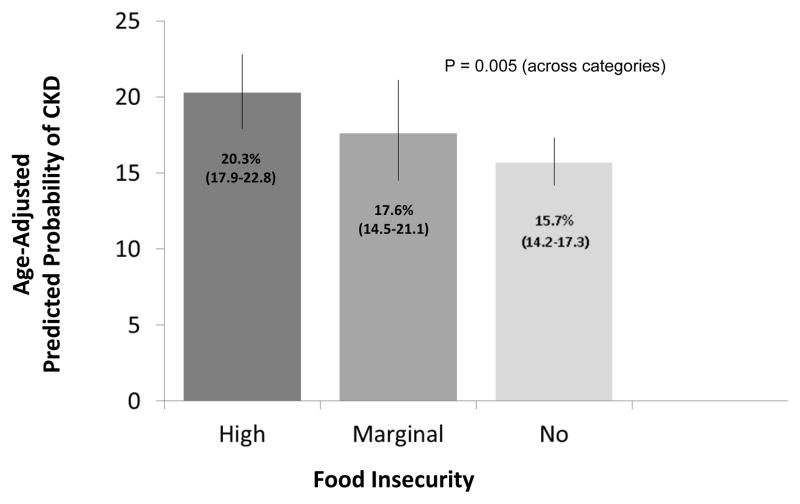
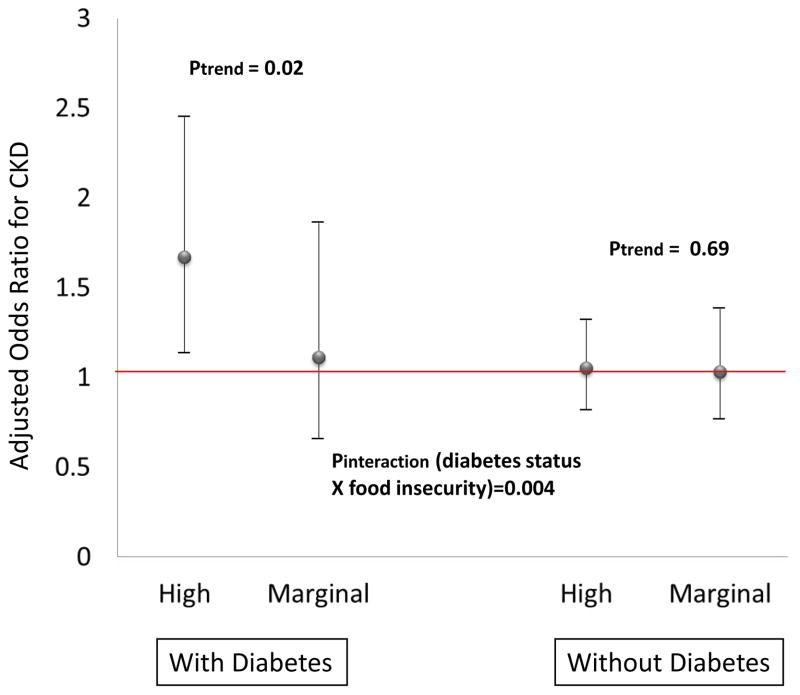
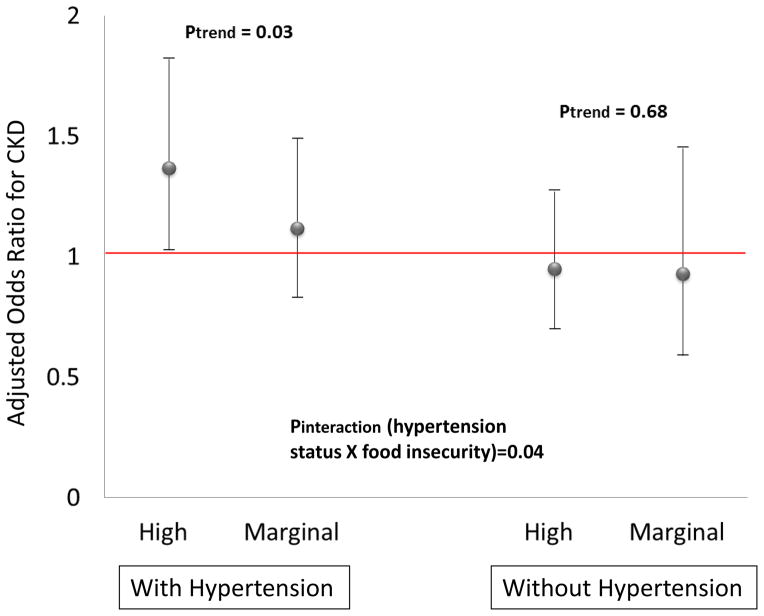
Results: In NHANES, the age-adjusted prevalence of CKD was 20.3, 17.6, and 15.7% for the high, marginal, and no food insecurity groups, respectively. Analyses adjusting for sociodemographics and smoking status revealed high food insecurity to be associated with greater odds of CKD only among participants with either diabetes (OR = 1.67, 95% CI: 1.14-2.45 comparing high to no food insecurity groups) or hypertension (OR = 1.37, 95% CI: 1.03-1.82). In HANDLS, the age-adjusted CKD prevalence was 5.9 and 4.6% for those with and without food insecurity, respectively (p = 0.33). Food insecurity was associated with a trend towards greater odds of CKD (OR = 1.46, 95% CI: 0.98-2.18) with no evidence of effect modification across diabetes, hypertension, or obesity subgroups.
Conclusion: Food insecurity may contribute to disparities in kidney disease, especially among persons with diabetes or hypertension, and is worthy of further study.
Figures
References
-
- Sabanayagam C, Shankar A, Saw SM, Lim SC, Tai ES, Wong TY. Socioeconomic status and microalbuminuria in an Asian population. Nephrol Dial Transplant. 2009;24:123–129. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
