

Review
doi: 10.1038/nrg3563.
Pluripotent stem cells in regenerative medicine: challenges and recent progress
Affiliations
- PMID: 24434846
- PMCID: PMC4539940
- DOI: 10.1038/nrg3563
Item in Clipboard
Review
Pluripotent stem cells in regenerative medicine: challenges and recent progress
Nat Rev Genet.
2014 Feb.
Abstract
After years of incremental progress, several recent studies have succeeded in deriving disease-relevant cell types from human pluripotent stem cell (hPSC) sources. The prospect of an unlimited cell source, combined with promising preclinical data, indicates that hPSC technology may be on the verge of clinical translation. In this Review, we discuss recent progress in directed differentiation, some of the new technologies that have facilitated the success of hPSC therapies and the remaining hurdles on the road towards developing hPSC-based cell therapies.
Figures
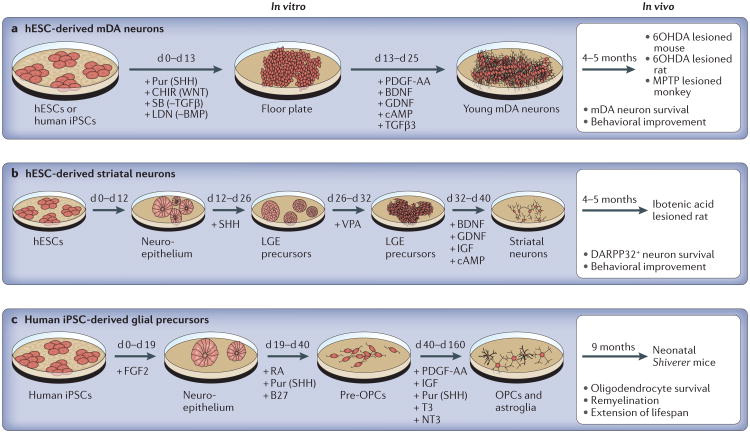
Schematic diagrams show published protocols for the generation of midbrain dopamine (mDA) neurons for the potential treatment of Parkinson's disease, striatal neurons for the treatment of Huntington's disease and glial precursors for the treatment of demyelinating disorders. Small molecules and growth factors that are used to direct cell fate are indicated below the arrows; the factors that are induced or inhibited are shown in parentheses. All studies showed robust long-term in vivo survival and functional improvement in at least one relevant animal model of disease. Although protocols for generating mDA neurons are relatively fast and efficient, protocols for generating oligodendrocyte precursor cells (OPCs) can take more than five months of in vitro differentiation. a. To differentiate human pluripotent stem cells (hPSCs) into mDA neurons through a floor plate intermediate, combined induction of neural floor plate using four small molecules from day 0 to day 13 (d 0–d 13) is followed by neuronal differentiation in the presence of a ‘cocktail’ of growth factors that promote mDA neuron fate. Cells are ready for transplantation into rodent or primate models of Parkinson's disease by day 25 of differentiation, which corresponds to the stage at which mDA neurons are born but still immature. b. To differentiate human embryonic stem cells (hESCs) into striatal neurons, neural induction into the neural rosette stage (that is, the neuroepithelium) is followed by exposure to a precise concentration of sonic hedgehog (SHH), which is required to specifically induce striatal precursors that emerge from the lateral ganglionic eminence (LGE) region during development. Floating cultures of LGE precursors are replated and further matured into striatal neurons. By day 40, these neurons are transplanted into a striatal lesion model of Huntington's disease. DARPP32 is a marker for spiny neurons. c. To differentiate human induced pluripotent stem cells (iPSCs) into glial precursors, neuroepithelial cells are isolated and treated with factors that promote ventral cell fates, followed by a protracted period of in vitro proliferation and maturation to obtain OPCs that are capable of efficient in vivo myelination. 6OHDA, 6-hydroxydopamine; BDNF, brain-derived neurotrophic factor; BMP, bone morphogenetic protein; cAMP, cyclic AMP; CHIR, CHIR99021 (a small-molecule inhibitor); FGF2, fibroblast growth factor 2; GDNF, glial cell-derived neurotrophic factor; IGF, insulinlike growth factor; LDN, LDN193189 (a small-molecule inhibitor); MPTP, 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine; NT3, neurotrophin 3; PDGF-AA, platelet-derived growth factor AA; pur, puromycin; RA, retinoic acid; SB, SB431542 (a small-molecule inhibitor); T3, tri-iodothyronine; TGFβ, transforming growth factor-β; VPA, valproic acid.
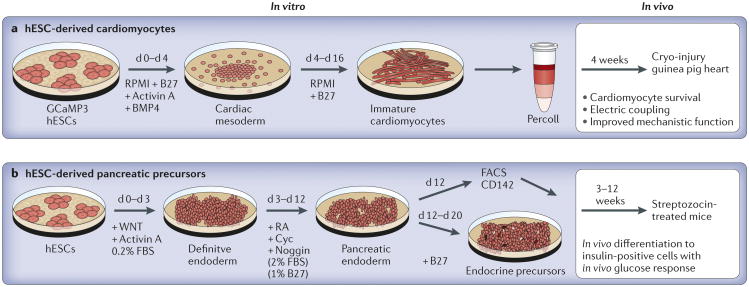
Schematic diagrams show published protocols for generating cardiomyocytes as an example of a mesodermal lineage with therapeutic potential and for generating pancreatic precursors as a key endodermal derivative that is crucial for clinical translation. Small molecules and growth factors that are used to direct cell fate are indicated below the arrows. Protocols for both lineages are rather short and require an enrichment step before transplantation. a. In the generation of cardiomyocytes from human embryonic stem cells (hESCs), a critical step is the induction of cardiac mesoderm in the presence of molecules that activate both bone morphogenetic protein (BMP) and Nodal– activin–transforming growth factor-β (TGFβ) signalling. Immature cardiomyocytes emerge by day 10 (d 10) of differentiation and are isolated by day 16. They are purified using Percoll, which is a physical separation technique. A critical step for the generation of cardiac cells is to show their ability to electrically couple with the host heart, as demonstrated using a genetic indicator of calcium signalling (GCaMP3). b. In the generation of hESC-derived pancreatic precursors,, induction of the endoderm is achieved in the presence of molecules that trigger WNT and Nodal–activin–TGFβ signalling pathways. Pancreatic endoderm is obtained by day 12 of differentiation, the stage at which cells can be either further matured in vitro or directly transplanted in vivo. Although in vivo maturation of CD142+ cells results in a large number of insulin-positive cells with appropriate glucose response, current techniques for in vitro maturation do not yield cells with proper glucose responsiveness. Cyc, cyclopamine; FACS, fluorescence-activated cell sorting; FBS, fetal bovine serum; RA, retinoic acid.
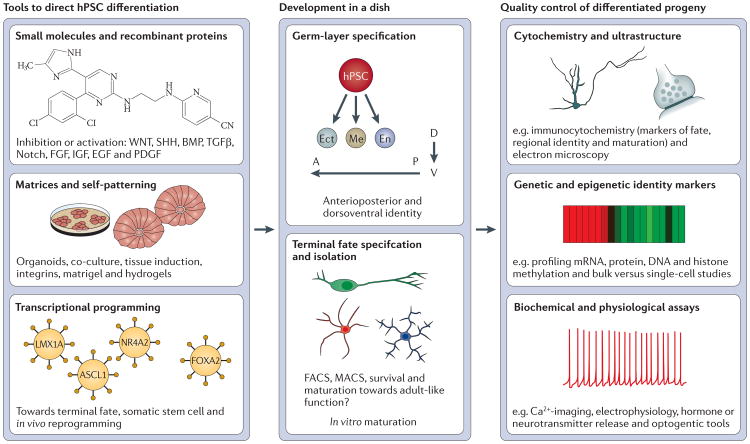
The key tools that are used to direct the differentiation of human pluripotent stem cells (hPSCs) to somatic cell types are shown. The use of small-molecule-based approaches has been particularly useful in generating cells with potential therapeutic relevance. Most strategies for directed cell differentiation are based on recreating aspects of normal development in vitro. One key developmental decision during the differentiation of hPSCs is the initial specification towards one of the three germ layer derivatives (that is, lineages of the ectoderm (ect), endoderm (en) or mesoderm (me)). A second crucial decision for hPSCs is to acquire specific anterioposterior (A–P) and dorsoventral (D–V) patterning fates. By recreating those specific signalling conditions, it is possible to generate hPSC-derived lineages that correspond to the cells that originate in the different regions of the developing embryo. However, despite such progress, a limited understanding of human development and its protracted timeframes remain important ‘roadblocks’ in the field. Assessment of the authenticity of cell fate in the differentiated progeny is a crucial element of any directed differentiation strategy. In addition to traditional methods such as cytochemistry and gene expression studies, there is an increased need for robust in vitro functional assays. ASCL1, achaete-scute homologue 1; BMP, bone morphogenetic protein; EGF, epidermal growth factor; FACS, fluorescence-activated cell sorting; FGF, fibroblast growth factor; FOXA2, forkhead box protein A2; IGF, insulin-like growth factor; LMX1A, LIM homeobox transcription factor 1-α; MACS, magnetic activated cell sorting; NR4A2, nuclear receptor subfamily 4 group A member 2; PDGF, platelet-derived growth factor; SHH, sonic hedgehog; TGFβ, transforming growth factor-β.
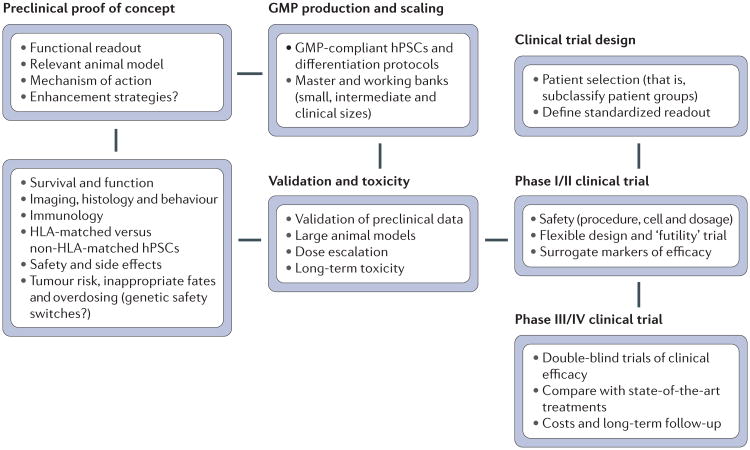
To move human pluripotent stem cell (hPSC)-derived cells from the bench to clinical studies, some key steps and challenges need to be addressed. Following a preclinical proof of concept, it is important to validate robustness in relevant disease models and to develop a cell-manufacturing strategy that is suitable for clinical translation. Important steps include producing cells at a sufficient scale (that is, creating a cell bank) and using fully standardized protocols under current good manufacturing practice (GMP)-compliant conditions. The resulting bank of the candidate therapeutic cell product needs to be revalidated for safety and efficacy before it can be considered as a candidate clinical product for early safety studies, and eventually efficacy studies, in human patients. HLA, human leukocyte antigen.
References
-
- Bellin M, Marchetto MC, Gage FH, Mummery CL. Induced pluripotent stem cells: the new patient? Nature Rev Mol Cell Biol. 2012;13:713–726. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
