

Practice Variance, Prevalence, and Economic Burden of Premature Infants Diagnosed With GERD
- PMID: 24435191
- PMCID: PMC4075760
- DOI: 10.1542/hpeds.2013-0036
Practice Variance, Prevalence, and Economic Burden of Premature Infants Diagnosed With GERD
Abstract
Objective: To determine the practice variance, prevalence, and economic burden of clinically diagnosed gastroesophageal reflux disease (GERD) in preterm infants.
Methods: Applying a retrospective cohort study design, we analyzed data from 18 567 preterm infants of 22 to 36 weeks' gestation and >400 g birth weight from the NICUs of 33 freestanding children's hospitals in the United States. GERD prevalence, comorbidities, and demographic factors were examined for their association with average length of stay (LOS) and hospitalization cost.
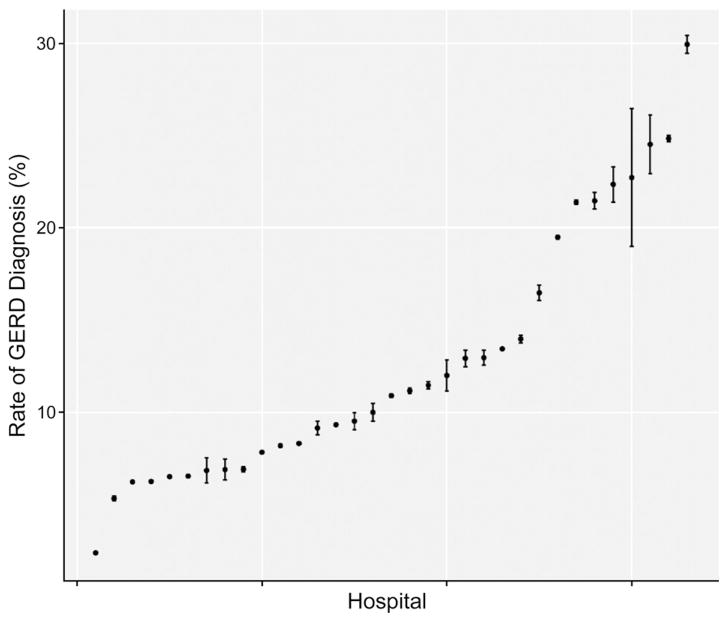
Results: Overall, 10.3% of infants received a diagnosis of GERD (95% confidence interval [CI]: 9.8-10.7). There was a 13-fold variation in GERD rates across hospitals (P < .001). GERD diagnosis was significantly (P < .05) associated with bronchopulmonary dysplasia and necrotizing enterocolitis, as well as congenital anomalies and decreased birth weight. GERD diagnosis was associated with $70 489 (95% CI: 62 184-78 794) additional costs per discharge and 29.9 additional days in LOS (95% CI: 27.3-32.5).
Conclusions: One in 10 of these premature NICU infants were diagnosed with GERD, which is associated with substantially increased LOS and elevated costs. Better diagnostic and management strategies are needed to evaluate reflux-type symptoms in this vulnerable NICU population.
Keywords: GERD; economic burden; length of stay; neonate.
Conflict of interest statement
Figures
References
-
- Vandenplas Y, Rudolph CD, Di Lorenzo C, et al. North American Society for Pediatric Gastroenterology Hepatology and Nutrition; European Society for Pediatric Gastroenterology Hepatology and Nutrition. Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) J Pediatr Gastroenterol Nutr. 2009;49(4):498–547. - PubMed
-
- Jadcherla SR. Esophageal motility in the human neonate. Neoreviews. 2006;7(1):e7–e12.
-
- Jadcherla SR, Gupta A, Fernandez S, et al. Spatiotemporal characteristics of acid refluxate and relationship to symptoms in premature and term infants with chronic lung disease. Am J Gastroenterol. 2008;103(3):720–728. - PubMed
-
- Hassall E. Over-prescription of acid-suppressing medications in infants: how it came about, why it’s wrong, and what to do about it. J Pediatr. 2012;160(2):193–198. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
