

One-year mortality and predictors of death among hospital survivors of acute respiratory distress syndrome
- PMID: 24435201
- PMCID: PMC3943651
- DOI: 10.1007/s00134-013-3186-3
One-year mortality and predictors of death among hospital survivors of acute respiratory distress syndrome
Abstract
Purpose: Advances in supportive care and ventilator management for acute respiratory distress syndrome (ARDS) have resulted in declines in short-term mortality, but risks of death after survival to hospital discharge have not been well described. Our objective was to quantify the difference between short-term and long-term mortality in ARDS and to identify risk factors for death and causes of death at 1 year among hospital survivors.
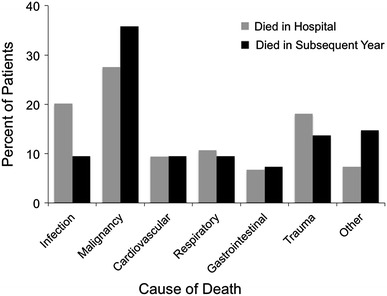
Methods: This multi-intensive care unit, prospective cohort included patients with ARDS enrolled between January 2006 and February 2010. We determined the clinical characteristics associated with in-hospital and 1-year mortality among hospital survivors and utilized death certificate data to identify causes of death.
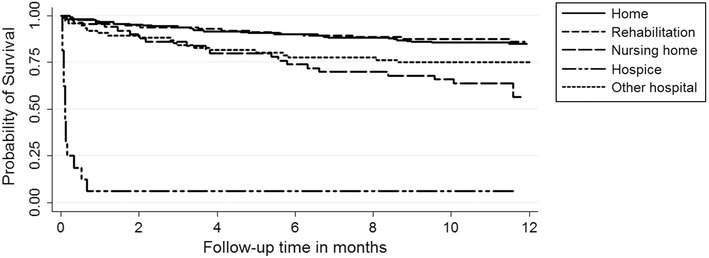
Results: Of 646 patients hospitalized with ARDS, mortality at 1 year was substantially higher (41 %, 95% CI 37-45%) than in-hospital mortality (24%, 95% CI 21-27%), P < 0.0001. Among 493 patients who survived to hospital discharge, the 110 (22%) who died in the subsequent year were older (P < 0.001) and more likely to have been discharged to a nursing home, other hospital, or hospice compared to patients alive at 1 year (P < 0.001). Important predictors of death among hospital survivors were comorbidities present at the time of ARDS, and not living at home prior to admission. ARDS-related measures of severity of illness did not emerge as independent predictors of mortality in hospital survivors.
Conclusions: Despite improvements in short-term ARDS outcomes, 1-year mortality is high, mostly because of the large burden of comorbidities, which are prevalent in patients with ARDS.
Figures
Comment in
-
Improved ICU outcomes in ARDS patients: implication on long-term outcomes.Intensive Care Med. 2014 Mar;40(3):448-50. doi: 10.1007/s00134-013-3200-9. Epub 2014 Jan 17. Intensive Care Med. 2014. PMID: 24435204 No abstract available.
References
-
- The Acute Respiratory Distress Syndrome Network Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–1308. - PubMed
-
- Antonelli M, Conti G, Esquinas A, Montini L, Maggiore SM, Bello G, Rocco M, Maviglia R, Pennisi MA, Gonzalez-Diaz G, Meduri GU. A multiple-center survey on the use in clinical practice of noninvasive ventilation as a first-line intervention for acute respiratory distress syndrome. Crit Care Med. 2007;35:18–25. doi: 10.1097/01.CCM.0000251821.44259.F3. - DOI - PubMed
-
- Piquilloud L, Tassaux D, Bialais E, Lambermont B, Sottiaux T, Roeseler J, Laterre PF, Jolliet P, Revelly JP. Neurally adjusted ventilatory assist (NAVA) improves patient-ventilator interaction during non-invasive ventilation delivered by face mask. Intensive Care Med. 2012;38:1624–1631. doi: 10.1007/s00134-012-2626-9. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- KL2 TR000143/TR/NCATS NIH HHS/United States
- MCRR/NIH UL1 RR024975-01/PHS HHS/United States
- NHLBI HL081332/PHS HHS/United States
- R01 HL051856/HL/NHLBI NIH HHS/United States
- K24 HL103836/HL/NHLBI NIH HHS/United States
- NHLBI HL090833/PHS HHS/United States
- NHLBI 1K23HL116800-01/PHS HHS/United States
- K23 HL116800/HL/NHLBI NIH HHS/United States
- T32 HL087738/HL/NHLBI NIH HHS/United States
- UL1 RR024975/RR/NCRR NIH HHS/United States
- R01 HL110969/HL/NHLBI NIH HHS/United States
- HL103836/HL/NHLBI NIH HHS/United States
- UL1 TR000445/TR/NCATS NIH HHS/United States
- HL110969/HL/NHLBI NIH HHS/United States
- UCSF-CTSI KL2 TR000143/TR/NCATS NIH HHS/United States
- NHLBI HL51856/PHS HHS/United States
- R37 HL051856/HL/NHLBI NIH HHS/United States
- U01 HL081332/HL/NHLBI NIH HHS/United States
- K23 HL090833/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
