

Prone positioning reduces mortality from acute respiratory distress syndrome in the low tidal volume era: a meta-analysis
- PMID: 24435203
- PMCID: PMC3976426
- DOI: 10.1007/s00134-013-3194-3
Prone positioning reduces mortality from acute respiratory distress syndrome in the low tidal volume era: a meta-analysis
Abstract
Purpose: Prone positioning for ARDS has been performed for decades without definitive evidence of clinical benefit. A recent multicenter trial demonstrated for the first time significantly reduced mortality with prone positioning. This meta-analysis was performed to integrate these findings with existing literature and test whether differences in tidal volume explain conflicting results among randomized trials.
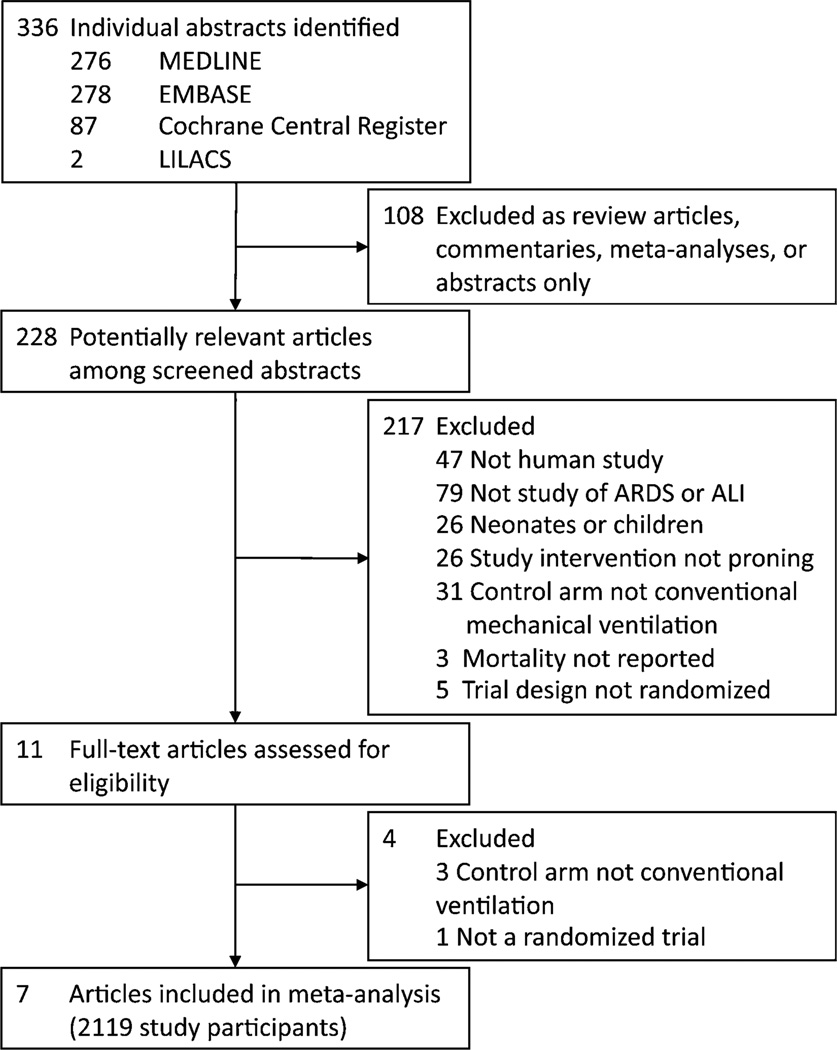
Methods: Studies were identified using MEDLINE, EMBASE, Cochrane Register of Controlled Trials, LILACS, and citation review. Included were randomized trials evaluating the effect on mortality of prone versus supine positioning during conventional ventilation for ARDS. The primary outcome was risk ratio of death at 60 days meta-analyzed using random effects models. Analysis stratified by high (>8 ml/kg predicted body weight) or low (≤ 8 ml/kg PBW) mean baseline tidal volume was planned a priori.
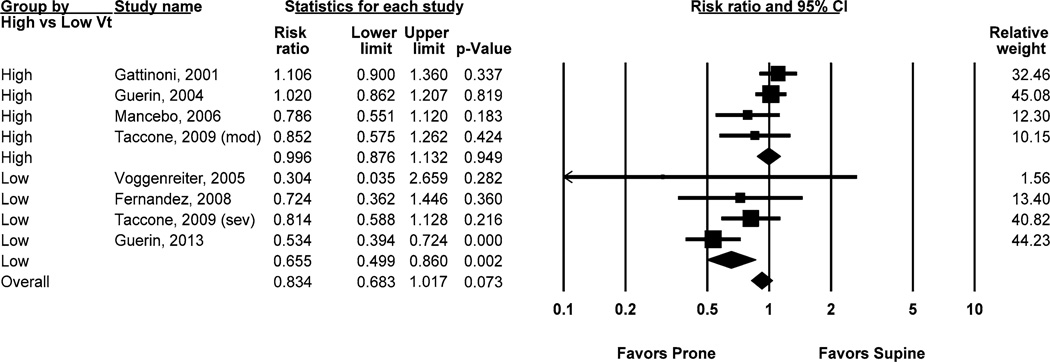
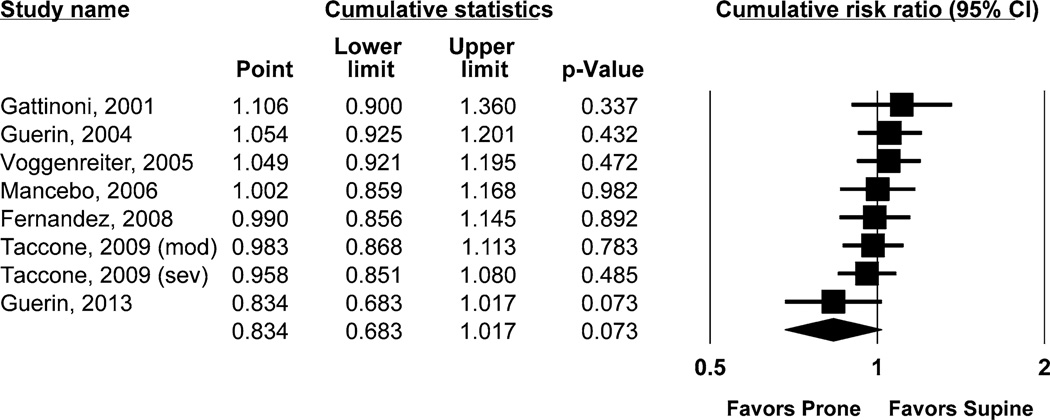
Results: Seven trials were identified including 2,119 patients, of whom 1,088 received prone positioning. Overall, prone positioning was not significantly associated with the risk ratio of death (RR 0.83; 95% CI 0.68-1.02; p = 0.073; I (2) = 64%). When stratified by high or low tidal volume, prone positioning was associated with a significant decrease in RR of death only among studies with low baseline tidal volume (RR 0.66; 95% CI 0.50-0.86; p = 0.002; I (2) = 25%). Stratification by tidal volume explained over half the between-study heterogeneity observed in the unstratified analysis.
Conclusions: Prone positioning is associated with significantly reduced mortality from ARDS in the low tidal volume era. Substantial heterogeneity across studies can be explained by differences in tidal volume.
Conflict of interest statement
Figures
References
-
- Rubenfeld GD, Caldwell E, Peabody E, et al. Incidence and outcomes of acute lung injury. N Engl J Med. 2005;353:1685–1693. - PubMed
-
- Brower RG, Matthay MA, Morris A, et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–1308. - PubMed
-
- Papazian L, Forel JM, Gacouin A, et al. Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med. 2010;363:1107–1116. - PubMed
-
- ARDS Definition Task Force. Ranieri VM, Rubenfeld GD, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307:2526–2533. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
