

Clinical correlates of insulin sensitivity and its association with mortality among men with CKD stages 3 and 4
- PMID: 24436478
- PMCID: PMC3974352
- DOI: 10.2215/CJN.05230513
Clinical correlates of insulin sensitivity and its association with mortality among men with CKD stages 3 and 4
Abstract
Background and objectives: Insulin resistance participates in the pathogenesis of multiple metabolic and cardiovascular diseases. CKD patients have impaired insulin sensitivity, but the clinical correlates and outcome associations of impaired insulin sensitivity in this vulnerable population are not well defined.
Design, setting, participants, & measurements: The prospective cohort study was from the third examination cycle of the Uppsala Longitudinal Study of Adult Men, a population-based survey of elderly men ages 70-71 years; insulin sensitivity was assessed by glucose disposal rate as measured with euglycemic clamps. Inclusion criterion was eGFR<60 ml/min per 1.73 m(2) (n=543). Exclusion criteria were incomplete data on euglycemic clamp and diabetes (n=97), leaving 446 men with CKD stages 3 and 4 (eGFR median=51.9 ml/min per 1.73 m(2); range=20.2-59.5 ml/min per 1.73 m(2)).
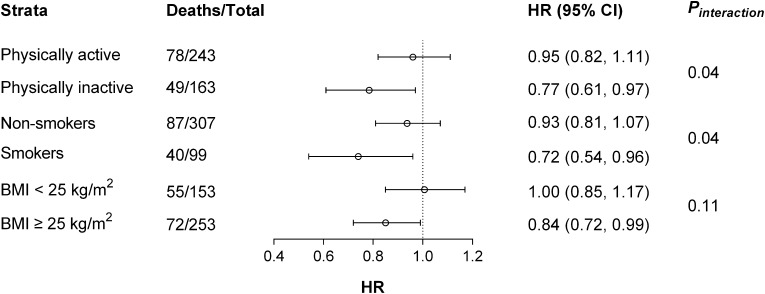
Results: The mean of glucose disposal rate was 5.4 ± 1.9 mg/kg per minute. In multivariable analysis, the independent clinical correlates of glucose disposal rate were eGFR (slope, 0.02; 95% confidence interval, 0.01 to 0.04), hypertension (-0.48; 95% confidence interval, -0.86 to -0.11), hyperlipidemia (-0.51; 95% confidence interval, -0.84 to -0.18), and body mass index (-0.32; 95% confidence interval, -0.37 to -0.27). During follow-up (median=10.0 years; interquartile range=8.7-11.0 years), 149 participants died. In Cox regression models, glucose disposal rate was not associated with all-cause or cardiovascular mortality. Multiplicative interactions (P<0.05) were observed between glucose disposal rate and physical activity or smoking in total mortality association. After subsequent stratification, glucose disposal rate was an independent correlate of all-cause mortality in smokers (adjusted hazard ratio, 0.72; 95% confidence interval, 0.54 to 0.96 per 1 mg/kg per minute glucose disposal rate increase) and physically inactive individuals (hazard ratio, 0.77; 95% confidence interval, 0.61 to 0.97) but not their counterparts.
Conclusion: eGFR, together with various components of the metabolic syndrome, contributed to explain the variance of insulin sensitivity in men with CKD stages 3 and 4. Insulin sensitivity was associated with a lower mortality risk in individuals who smoked and individuals who were physically inactive.
Figures
Comment in
-
Insulin resistance in CKD.Clin J Am Soc Nephrol. 2014 Apr;9(4):638-40. doi: 10.2215/CJN.01290214. Epub 2014 Mar 27. Clin J Am Soc Nephrol. 2014. PMID: 24677558 Free PMC article. No abstract available.
References
-
- Zethelius B, Lithell H, Hales CN, Berne C: Insulin sensitivity, proinsulin and insulin as predictors of coronary heart disease. A population-based 10-year, follow-up study in 70-year old men using the euglycaemic insulin clamp. Diabetologia 48: 862–867, 2005 - PubMed
-
- Rutter MK, Meigs JB, Sullivan LM, D’Agostino RB, Sr., Wilson PW: Insulin resistance, the metabolic syndrome, and incident cardiovascular events in the Framingham Offspring Study. Diabetes 54: 3252–3257, 2005 - PubMed
-
- Barr EL, Zimmet PZ, Welborn TA, Jolley D, Magliano DJ, Dunstan DW, Cameron AJ, Dwyer T, Taylor HR, Tonkin AM, Wong TY, McNeil J, Shaw JE: Risk of cardiovascular and all-cause mortality in individuals with diabetes mellitus, impaired fasting glucose, and impaired glucose tolerance: The Australian Diabetes, Obesity, and Lifestyle Study (AusDiab). Circulation 116: 151–157, 2007 - PubMed
-
- Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, Gordon DJ, Krauss RM, Savage PJ, Smith SC, Jr., Spertus JA, Costa F, American Heart Association. National Heart, Lung, and Blood Institute : Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 112: 2735–2752, 2005 - PubMed
-
- Shinohara K, Shoji T, Emoto M, Tahara H, Koyama H, Ishimura E, Miki T, Tabata T, Nishizawa Y: Insulin resistance as an independent predictor of cardiovascular mortality in patients with end-stage renal disease. J Am Soc Nephrol 13: 1894–1900, 2002 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
