

Review
doi: 10.1055/s-0033-1353483.
Vertebroplasty
Affiliations
- PMID: 24436552
- PMCID: PMC3773069
- DOI: 10.1055/s-0033-1353483
Item in Clipboard
Review
Vertebroplasty
Semin Intervent Radiol.
2013 Sep.
Abstract
Percutaneous vertebroplasty has become widely accepted as a safe and effective minimally invasive procedure for the treatment of painful vertebral body compression fractures refractory to medical therapy. In this article, the authors review the indications and contraindications for vertebroplasty, principles of appropriate patient selection, useful techniques to achieve optimal outcomes, and the potential risks and complications of the procedure.
Keywords: interventional radiology; kyphoplasty; osteoporosis; vertebral augmentation; vertebral compression fracture; vertebroplasty.
Figures
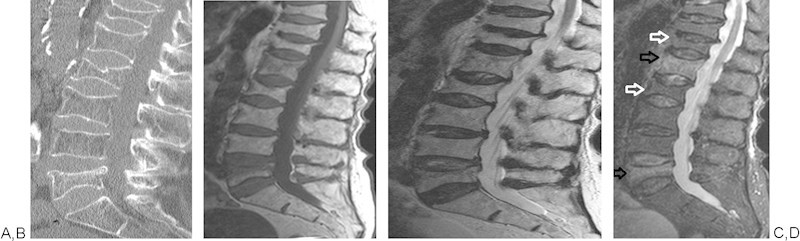
Sagittal CT reconstruction (A) showing multiple vertebral body fractures of unknown age. MRI T1, T2, and STIR images (B-D, respectively) confirm fractures, demonstrating marrow edema at L1 and L5 compatible with acute vertebral body fractures (black arrows). Lack of marrow edema at T12 and L2 suggests more chronic vertebral body fractures (white arrows).
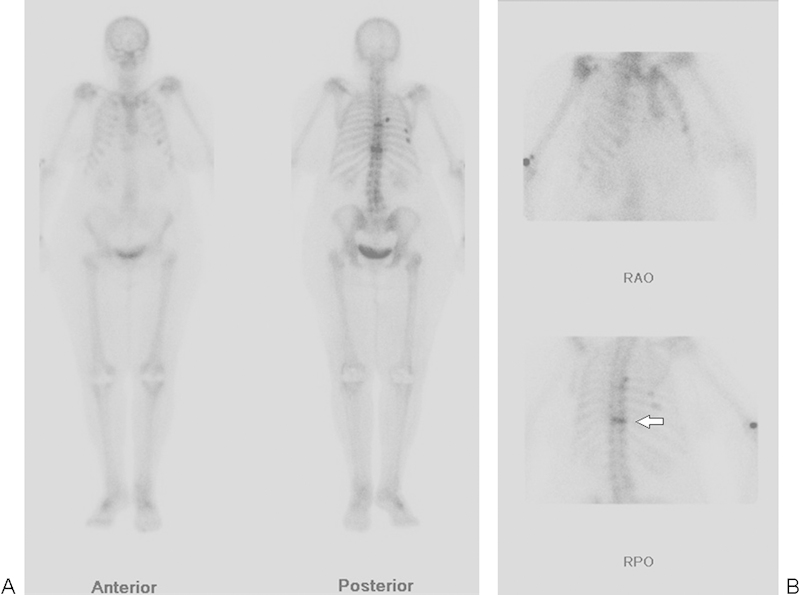
(A, B) Nuclear medicine bone scan, with anterior, posterior, right anterior oblique (RAO), and right posterior oblique (RPO) views, in a patient unable to have an MRI, showing increased radiotracer uptake at T10 consistent with an acute vertebral body fracture (arrow). Uptake is seen to a lesser degree at the mid-thoracic spine compatible with a second acute fracture. Multiple rib fractures are also present.
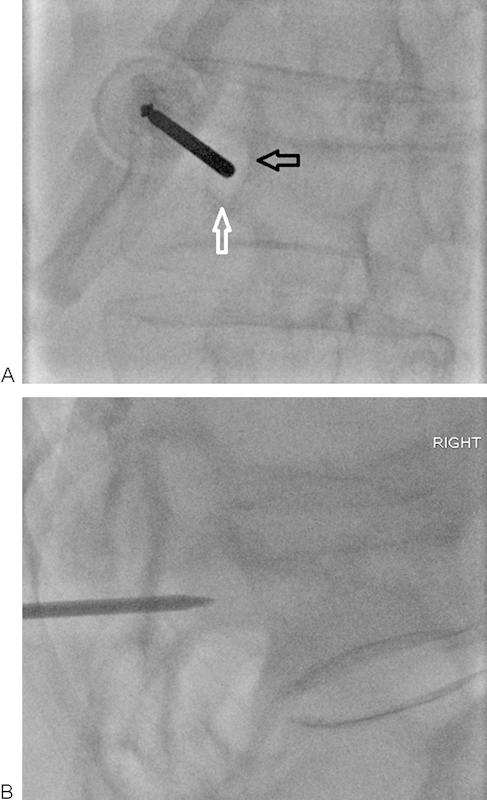
(A, B) Ipsilateral oblique and lateral fluoroscopic views of a T10 vertebral fracture. The needle should be advanced at the upper and outer quadrant of the pedicle. The needle must be advanced without violating the inferior (white arrow) and medial (black arrow) walls of the pedicle to avoid potential nerve or cord injury. Intermittent lateral views should be obtained to ensure appropriate angle of entry into the vertebral body.
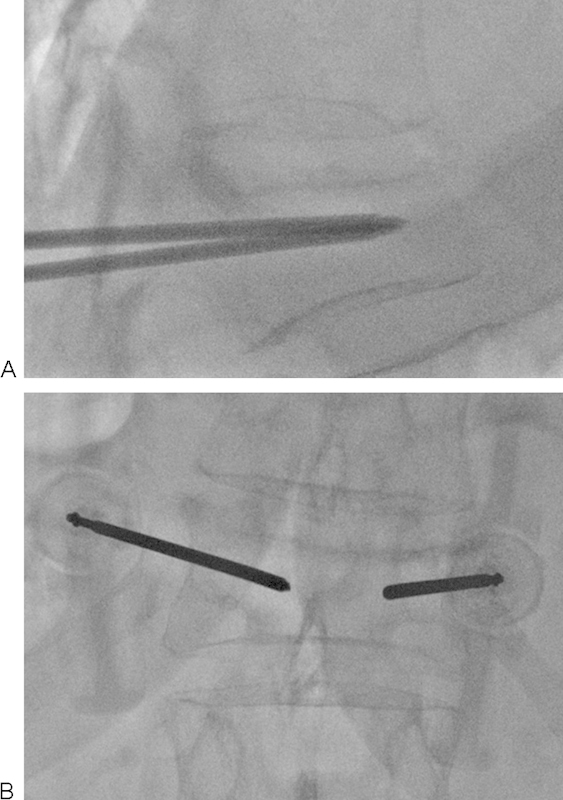
(A, B) Bilateral transpedicular access obtained for vertebroplasty. Needle positioning should be confirmed in both projections prior to the injection of cement. Ideally, the tips of the needles should be positioned as close to midline as possible at the junction of the anterior and middle third of the vertebral body.

(A, B) Satisfactory vertebroplasty endpoint with even distribution of cement.
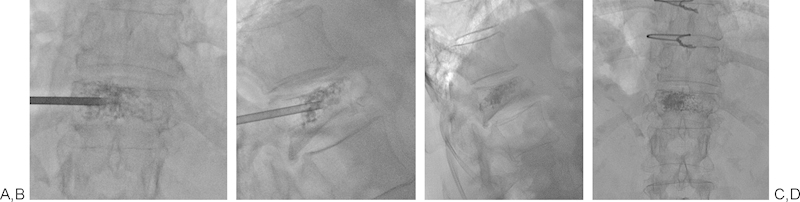
(A-D) Left unilateral transpedicular approach with ideal needle positioning and cement distribution.
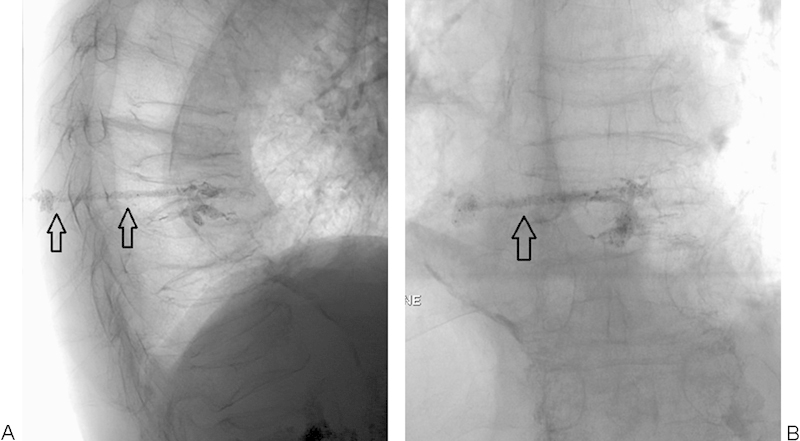
(A, B) Poorly filled mid-thoracic vertebral body after vertebroplasty. Notice the cement tail (black arrows) extending to the subcutaneous soft tissues. This can be avoided by clearing the needle of cement using the stylet, or by breaking the tail off by gently rocking and spinning the needle prior to removal. In this case, a small incision could be made to cut down on the tail and, using a hemostat, to physically remove as much as possible.
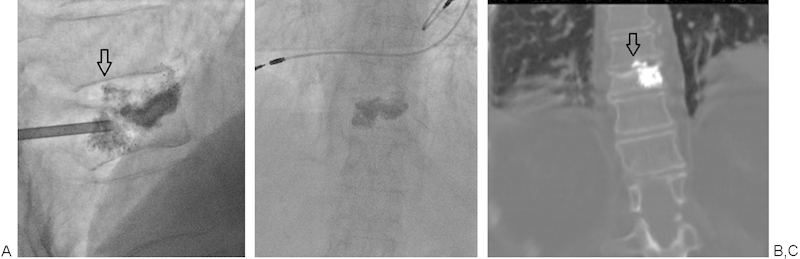
(A-C) Intradiscal extravasation of cement (arrows) in this case was asymptomatic, but uncommonly can be associated with pain. Cement injection should be paused when extravasation is encountered. Often waiting a minute or two will allow the cement more time to thicken and for the leak to seal.
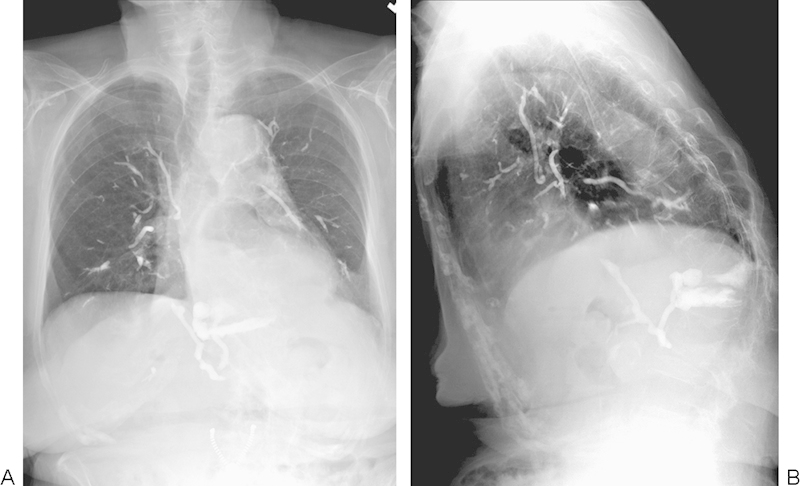
(A, B) A rare case of massive pulmonary emboli related to PMMA from a vertebroplasty performed in an outpatient setting. This patient survived, but eventually developed pulmonary hypertension. Images courtesy of Dr. Michael Jay.
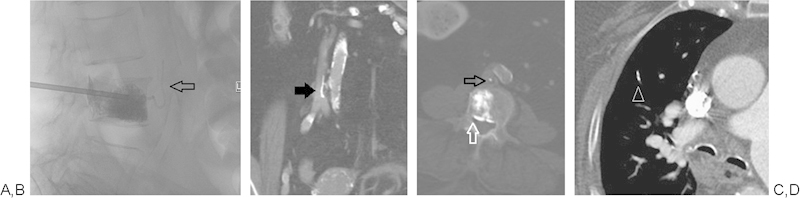
(A-D) Unipedicular vertebroplasty with extravasation of cement anteriorly via a vertebral vein and ultimately extending into the IVC (black arrows). Cement also extends beyond the posterior wall of the vertebral body and into epidural veins (white arrow). CT chest shows a small cement PE in the right middle lobe (white arrow head). The patient remained asymptomatic.
Similar articles
-
Vertebral augmentation.Handb Clin Neurol. 2021;176:379-394. doi: 10.1016/B978-0-444-64034-5.00017-1. Handb Clin Neurol. 2021. PMID: 33272406 Review.
-
Minding the Gap in Vertebroplasty: Vertebral Body Fracture Clefts and Cement Nonunion.Pain Physician. 2021 Mar;24(2):E221-E230. Pain Physician. 2021. PMID: 33740359
-
[Vertebroplasty and kyphoplasty : A critical statement].Radiologe. 2020 Feb;60(2):138-143. doi: 10.1007/s00117-020-00651-z. Radiologe. 2020. PMID: 31989205 Review. German.
-
Does Percutaneous Vertebroplasty or Balloon Kyphoplasty for Osteoporotic Vertebral Compression Fractures Increase the Incidence of New Vertebral Fractures? A Meta-Analysis.Pain Physician. 2017 Jan-Feb;20(1):E13-E28. Pain Physician. 2017. PMID: 28072794 Review.
-
Percutaneous vertebral augmentation: an elevation in adjacent-level fracture risk in kyphoplasty as compared with vertebroplasty.Spine J. 2007 Sep-Oct;7(5):575-82. doi: 10.1016/j.spinee.2006.10.020. Epub 2007 Jan 24. Spine J. 2007. PMID: 17905320
Cited by
-
Paraplegia due to intradural cement leakage after vertebroplasty: a case report and literature review.BMC Musculoskelet Disord. 2021 Aug 28;22(1):741. doi: 10.1186/s12891-021-04625-7. BMC Musculoskelet Disord. 2021. PMID: 34454446 Free PMC article. Review.
-
Cement augmentation for treatment of high to mid-thoracic osteoporotic compression fractures, high-viscosity cement percutaneous vertebroplasty versus balloon kyphoplasty.Sci Rep. 2022 Nov 12;12(1):19404. doi: 10.1038/s41598-022-22019-0. Sci Rep. 2022. PMID: 36371412 Free PMC article.
-
Percutaneous Vertebral Augmentation Techniques in Osteoporotic and Traumatic Fractures.Semin Intervent Radiol. 2018 Oct;35(4):309-323. doi: 10.1055/s-0038-1673639. Epub 2018 Nov 5. Semin Intervent Radiol. 2018. PMID: 30402014 Free PMC article. Review.
-
Comparative study of Lutetium-177 and Phosphorus-32 in radioactive bone cement for the treatment of vertebral body metastasis.J Cancer Res Clin Oncol. 2023 Aug;149(10):7479-7491. doi: 10.1007/s00432-023-04695-1. Epub 2023 Mar 24. J Cancer Res Clin Oncol. 2023. PMID: 36959343 Free PMC article.
-
Osteoporosis management-current and future perspectives - A systemic review.J Orthop. 2024 Mar 2;53:101-113. doi: 10.1016/j.jor.2024.03.002. eCollection 2024 Jul. J Orthop. 2024. PMID: 38495575 Free PMC article. Review.
References
-
- Leech J A, Dulberg C, Kellie S, Pattee L, Gay J. Relationship of lung function to severity of osteoporosis in women. Am Rev Respir Dis. 1990;141(1):68–71. - PubMed
-
- Borgström F, Zethraeus N, Johnell O. et al.Costs and quality of life associated with osteoporosis-related fractures in Sweden. Osteoporos Int. 2006;17(5):637–650. - PubMed
-
- Silverman S L. The clinical consequences of vertebral compression fracture. Bone. 1992;13 02:S27–S31. - PubMed
-
- Röllinghoff M, Zarghooni K, Schlüter-Brust K. et al.Indications and contraindications for vertebroplasty and kyphoplasty. Arch Orthop Trauma Surg. 2010;130(6):765–774. - PubMed
-
- Kado D M Browner W S Palermo L Nevitt M C Genant H K Cummings S R; Study of Osteoporotic Fractures Research Group. Vertebral fractures and mortality in older women: a prospective study Arch Intern Med 1999159111215–1220. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
