

Pelvic congestion syndrome
- PMID: 24436564
- PMCID: PMC3835435
- DOI: 10.1055/s-0033-1359731
Pelvic congestion syndrome
Abstract
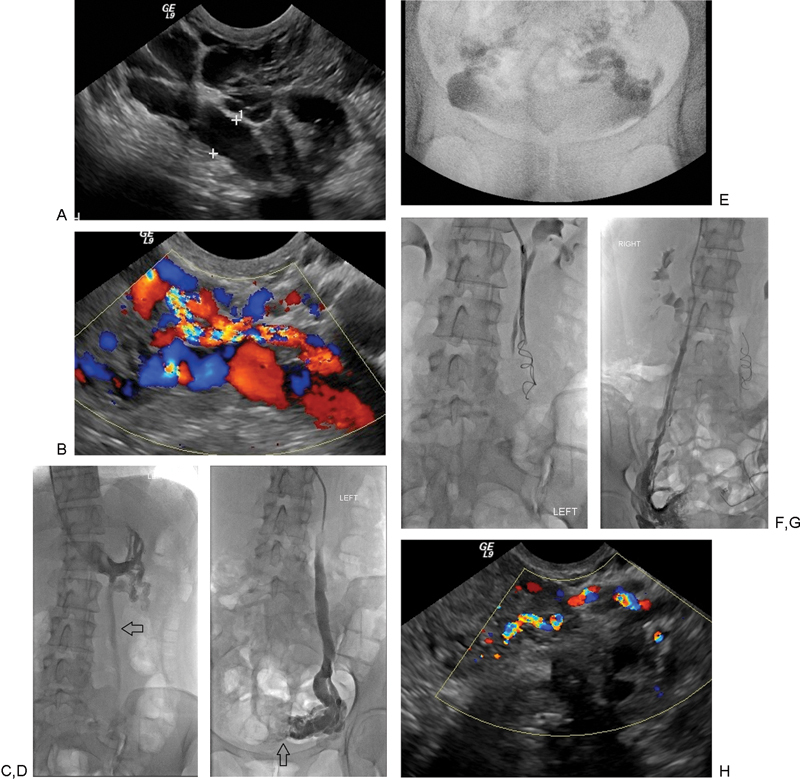
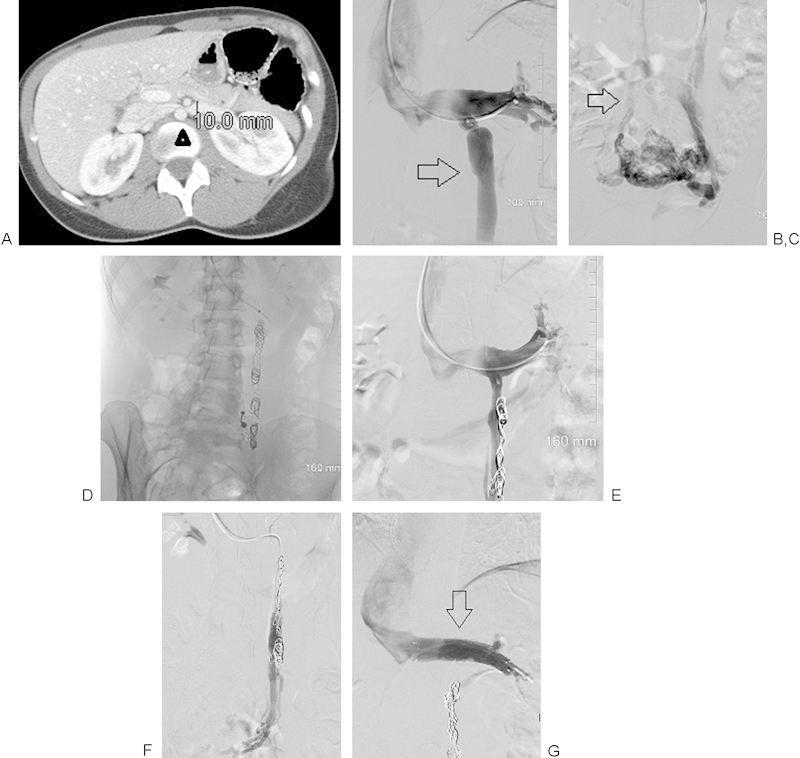
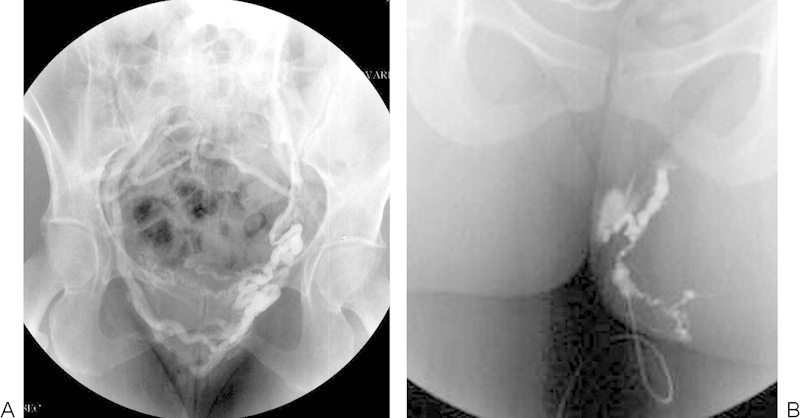
Patients with pelvic congestion syndrome present with otherwise unexplained chronic pelvic pain that has been present for greater than 6 months, and anatomic findings that include pelvic venous insufficiency and pelvic varicosities. It remains an underdiagnosed explanation for pelvic pain in young, premenopausal, usually multiparous females. Symptoms include noncyclical, positional lower back, pelvic and upper thigh pain, dyspareunia, and prolonged postcoital discomfort. Symptoms worsen throughout the day and are exacerbated by activity or prolonged standing. Examination may reveal ovarian tenderness and unusual varicosities-vulvoperineal, posterior thigh, and gluteal. Diagnosis is suspected by clinical history and imaging that demonstrates pelvic varicosities. Venography is usually necessary to confirm ovarian vein reflux, although transvaginal ultrasound may be useful in documenting this finding. Endovascular therapy has been validated by several large patient series with long-term follow-up using standardized pain assessment surveys. Embolization has been shown to be significantly more effective than surgical therapy in improving symptoms in patients who fail hormonal therapy. Although there has been variation in approaches between investigators, the goal is elimination of ovarian vein reflux with or without direct sclerosis of enlarged pelvic varicosities. Symptom reduction is seen in 70 to 90% of the treated females despite technical variation.
Keywords: female varicocele; nutcracker syndrome; pelvic congestion syndrome; pelvic pain syndrome; pelvic vascular congestion; pelvic vein incompetence; vulvar varices.
Figures
References
-
- Mathias S D, Kuppermann M, Liberman R F, Lipschutz R C, Steege J F. Chronic pelvic pain: prevalence, health-related quality of life, and economic correlates. Obstet Gynecol. 1996;87(3):321–327. - PubMed
-
- Farquhar C M, Rogers V, Franks S, Pearce S, Wadsworth J, Beard R W. A randomized controlled trial of medroxyprogesterone acetate and psychotherapy for the treatment of pelvic congestion. Br J Obstet Gynaecol. 1989;96(10):1153–1162. - PubMed
-
- Soysal M E, Soysal S, Vicdan K, Ozer S. A randomized controlled trial of goserelin and medroxyprogesterone acetate in the treatment of pelvic congestion. Hum Reprod. 2001;16(5):931–939. - PubMed
-
- Belenky A, Bartal G, Atar E, Cohen M, Bachar G N. Ovarian varices in healthy female kidney donors: incidence, morbidity, and clinical outcome. AJR Am J Roentgenol. 2002;179(3):625–627. - PubMed
-
- Ahlberg N E, Bartley O, Chidekel N. Right and left gonadal veins. An anatomical and statistical study. Acta Radiol Diagn (Stockh) 1966;4(6):593–601. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
