

Review
doi: 10.1055/s-0033-1359736.
Management of pulmonary arteriovenous malformations in hereditary hemorrhagic telangiectasia patients
Affiliations
- PMID: 24436569
- PMCID: PMC3835466
- DOI: 10.1055/s-0033-1359736
Item in Clipboard
Review
Management of pulmonary arteriovenous malformations in hereditary hemorrhagic telangiectasia patients
Semin Intervent Radiol.
2013 Dec.
No abstract available
Figures
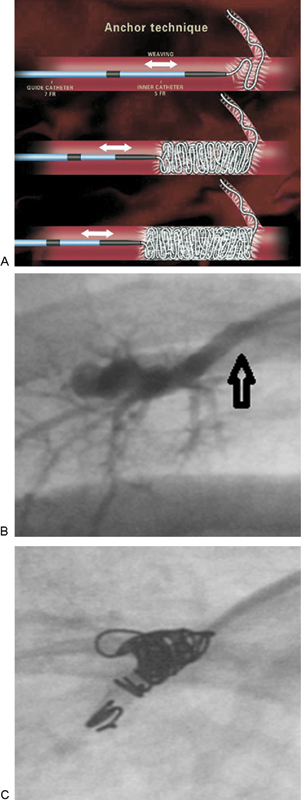
(A) Schematic demonstrating anchor coil technique to decrease the risk of distal migration of coils (reproduced with permission from White11) (B) A right lower lobe PAVM with a 3-mm feeding artery (arrow). (C) After deploying the first 2 cm of a 4-mm Nestor anchoring coil in a side branch, three additional coils were deployed safely. PAVM, pulmonary arteriovenous malformation.
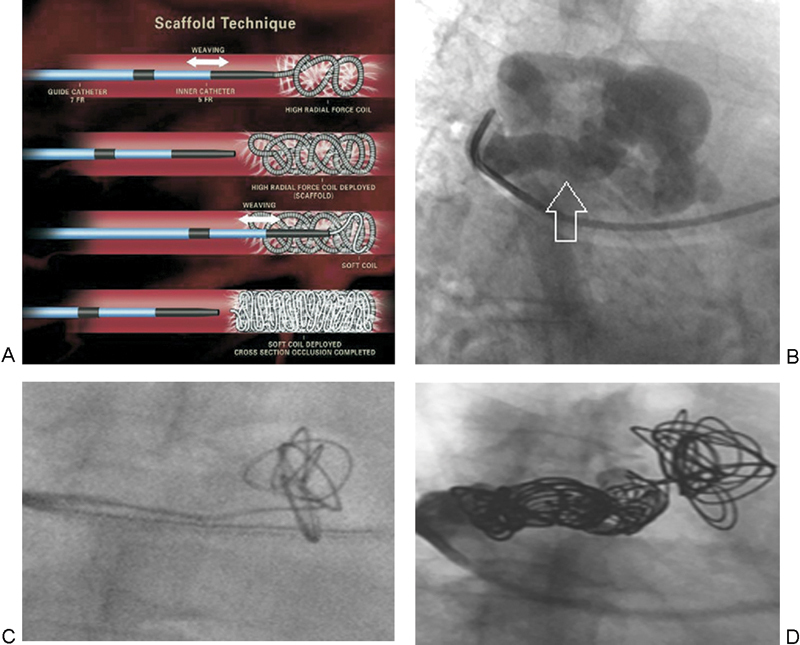
(A) Schematic demonstrating scaffold technique to decrease the risk of distal migration of coils (reproduced with permission from White11). (B) A right upper lobe PAVM with an 8-mm feeding artery (arrow). (C) A 10 mm × 26 cm stainless steel framing coil was deployed close to the aneurysm sac but within the feeding artery. (D) After deploying the framing coil, four additional coils were placed to tightly pack the matrix and achieve cross-sectional occlusion of the feeding artery. PAVM, pulmonary arteriovenous malformation.
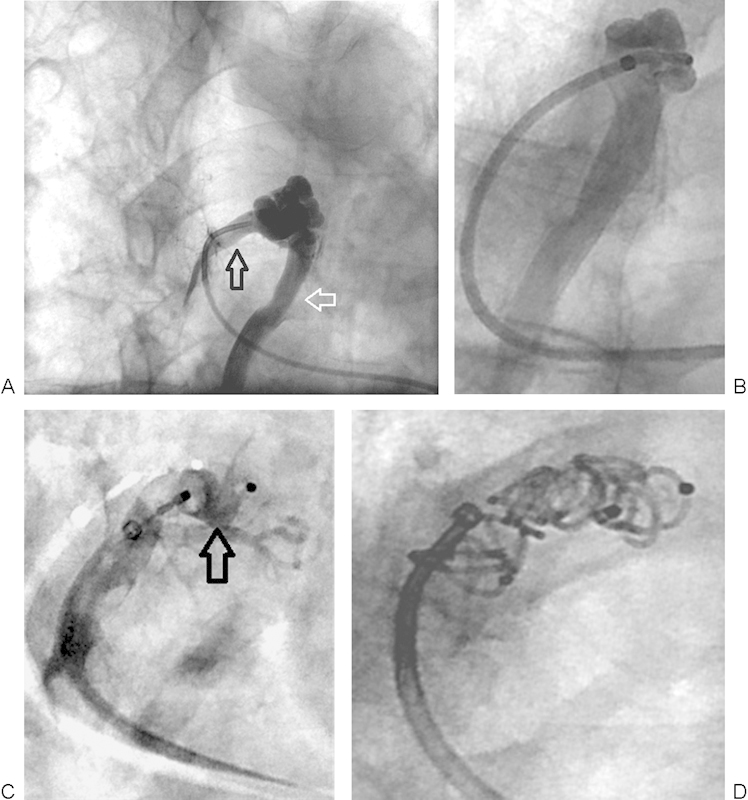
(A) Right upper lobe PAVM with 5-mm feeding artery (black arrow) and large draining vein (white arrow). (B) Successful negotiation of a 5-Fr guiding catheter into the distal feeding artery. The large draining vein is seen. (C) A 6-mm Amplatzer II vascular plug (arrow) was deployed close to the aneurysm sac but within the feeding artery. (D) After deploying the Amplatzer plug, five 5 mm × 5 cm coils were placed behind the plug to achieve cross-sectional occlusion of the feeding artery. PAVM, pulmonary arteriovenous malformation.
References
-
- Cottin V, Plauchu H, Bayle J-Y, Barthelet M, Revel D, Cordier J-F. Pulmonary arteriovenous malformations in patients with hereditary hemorrhagic telangiectasia. Am J Respir Crit Care Med. 2004;169(9):994–1000. - PubMed
-
- van Gent M WF, Post M C, Snijder R J, Westermann C JJ, Plokker H WM, Mager J J. Real prevalence of pulmonary right-to-left shunt according to genotype in patients with hereditary hemorrhagic telangiectasia: a transthoracic contrast echocardiography study. Chest. 2010;138(4):833–839. - PubMed
-
- Faughnan M E, Palda V A, Garcia-Tsao G. et al.International guidelines for the diagnosis and management of hereditary haemorrhagic telangiectasia. J Med Genet. 2011;48(2):73–87. - PubMed
-
- Gossage J R, Kanj G. Pulmonary arteriovenous malformations. A state of the art review. Am J Respir Crit Care Med. 1998;158(2):643–661. - PubMed
-
- Faughnan M E, Thabet A, Mei-Zahav M. et al.Pulmonary arteriovenous malformations in children: outcomes of transcatheter embolotherapy. J Pediatr. 2004;145(6):826–831. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
