

The Use of Intra-aortic Balloon Pump in a Real-World Setting: A Comparison between Survivors and Nonsurvivors from Acute Coronary Syndrome Treated with IABP. The Jakarta Acute Coronary Syndrome Registry
- PMID: 24436615
- PMCID: PMC3830567
- DOI: 10.1055/s-0033-1348884
The Use of Intra-aortic Balloon Pump in a Real-World Setting: A Comparison between Survivors and Nonsurvivors from Acute Coronary Syndrome Treated with IABP. The Jakarta Acute Coronary Syndrome Registry
Abstract
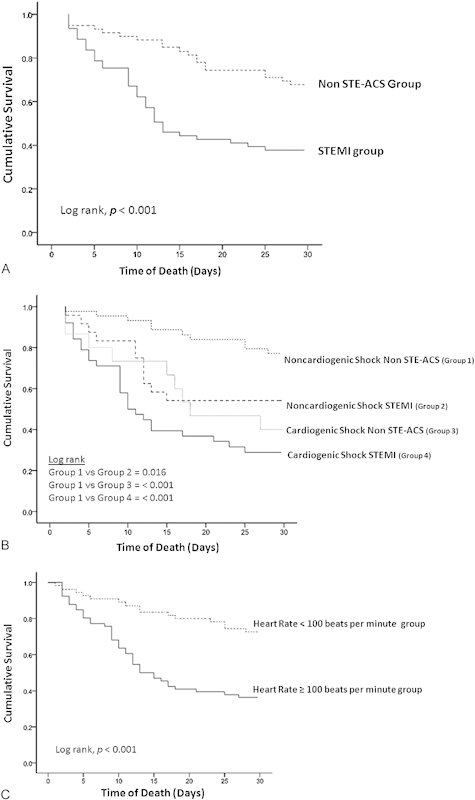
Real-world data on acute coronary syndrome (ACS) patients who received intra-aortic balloon pump (IABP) support are limited. The objective of this study was to evaluate the characteristics of ACS patients who received IABP support from a real-world ACS registry. Patients with ACS (N = 121) who received IABP support were enrolled. Characteristics of survivors and nonsurvivors were compared at 30 days. Mortality rate of patients with ACS who received IABP was 47%. The survivors (N = 64) had less often cardiogenic shock (p < 0.001), more often IABP usage as back-up for a revascularization procedure (p = 0.002), less often resuscitation (p = 0.043), and less mechanical ventilator support (p < 0.001) than nonsurvivors. The nonsurvivors had a significantly higher leukocyte count (p = 0.033), a higher serum creatinine level (p < 0.001), a higher blood sugar on admission (p = 0.001), higher creatine kinase MB levels (p = 0.002), and a higher serum uric acid level (p < 0.001), but significantly lower left and right ventricular function (p = 0.014 and p = 0.003, respectively) than survivors. At 30 days, non-ST elevation (STE)-ACS patients had lower mortality rate than ST segment elevation myocardial infarction patients (log-rank test, p < 0.001), and non-STE-ACS patients who had not suffered from cardiogenic shock showed the lowest mortality rate (log-rank test, p < 0.001). By multivariate analysis, a heart rate ≥ 100 beats per minute before IABP insertion was the strongest predictor of 30-day mortality (hazard ratio = 5.69; 95% confidence interval, 1.49 to 21.78; p = 0.011). In ACS patients presenting with either cardiogenic shock, resuscitated, or patients who needed mechanical ventilation suffered from high mortality, despite the use of IABP. IABP appears to be safe and tended to be favorable in noncardiogenic shock ACS patients, particularly non-STE-ACS. A heart rate of ≥ 100 beats per minute prior to IABP insertion was the strongest predictor of 30-day mortality.
Keywords: ACS; IABP; nonsurvivor; survivor.
Conflict of interest statement
Figures
References
-
- Kantrowitz A, Tjonneland S, Freed P S, Phillips S J, Butner A N, Sherman J L Jr. Initial clinical experience with intraaortic balloon pumping in cardiogenic shock. JAMA. 1968;203(2):113–118. - PubMed
-
- Weber K T, Janicki J S. Intraaortic balloon counterpulsation. A review of physiological principles, clinical results, and device safety. Ann Thorac Surg. 1974;17(6):602–636. - PubMed
-
- Scheidt S, Wilner G, Mueller H. et al.Intra-aortic balloon counterpulsation in cardiogenic shock. Report of a co-operative clinical trial. N Engl J Med. 1973;288(19):979–984. - PubMed
-
- Antman E M, Anbe D T, Armstrong P W. et al.American College of Cardiology; American Heart Association Task Force on Practice Guidelines; Canadian Cardiovascular Society . ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction) Circulation. 2004;110(9):e82–e292. - PubMed
-
- Levine G N, Bates E R, Blankenship J C. et al.ACCF; AHA; SCAI . 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Catheter Cardiovasc Interv. 2012;79(3):453–495. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
