

The sauvé-kapandji procedure
- PMID: 24436787
- PMCID: PMC3656576
- DOI: 10.1055/s-0032-1333465
The sauvé-kapandji procedure
Abstract
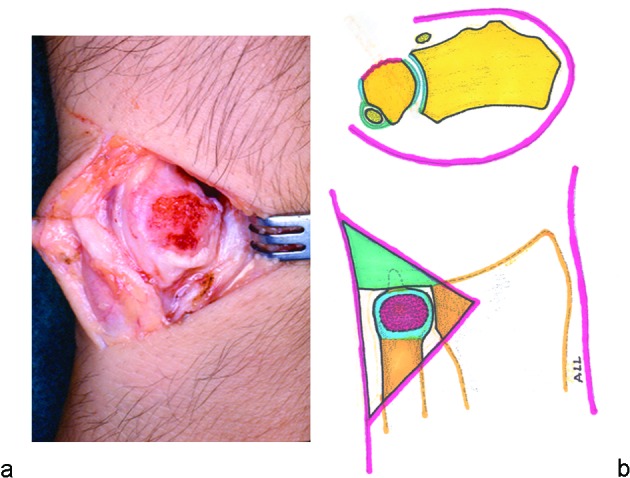
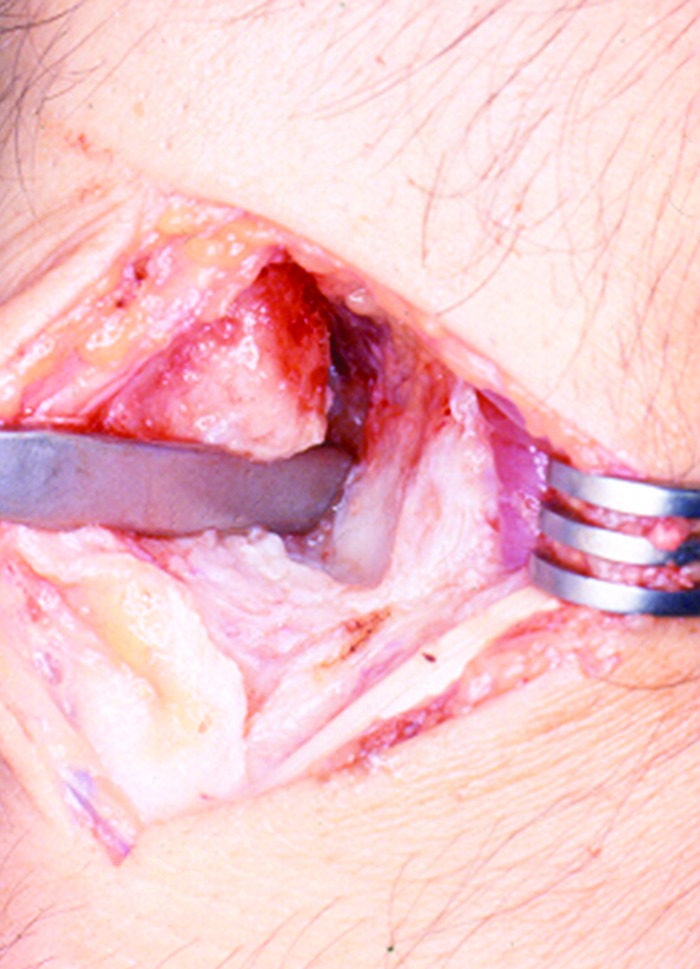
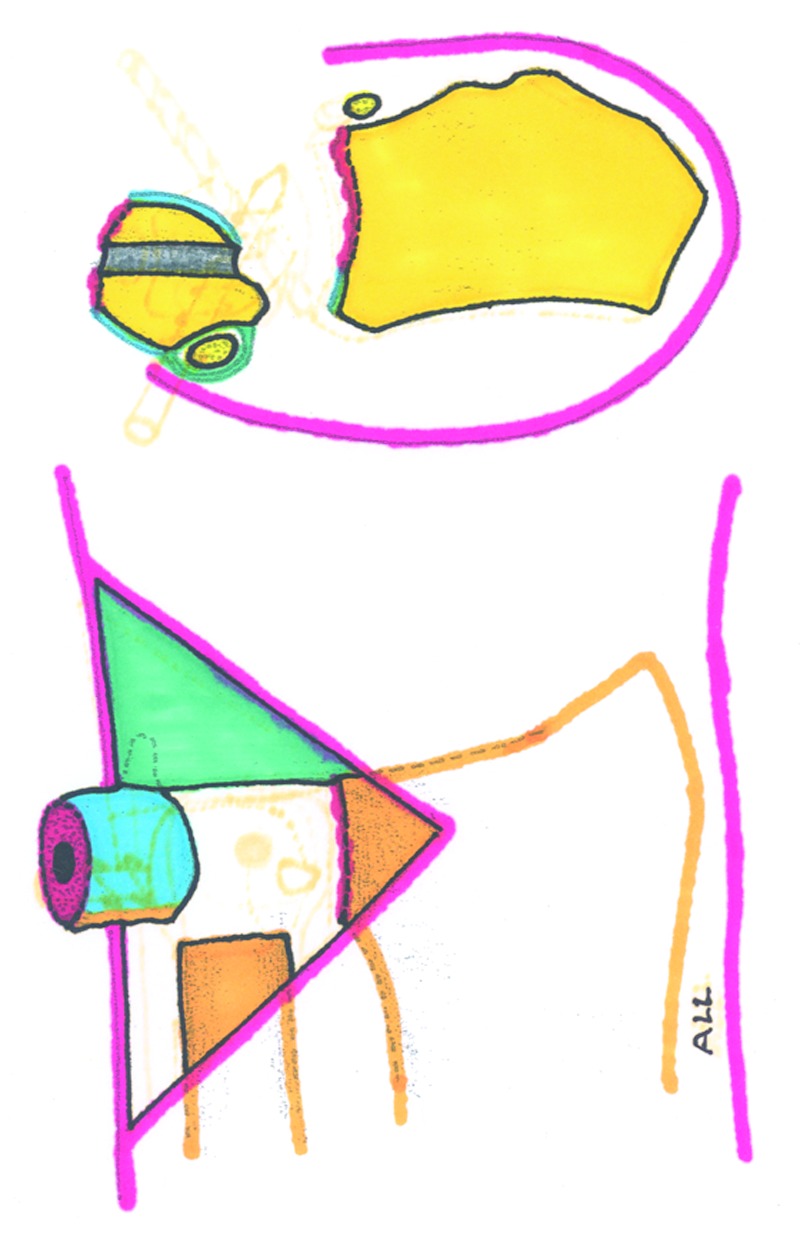
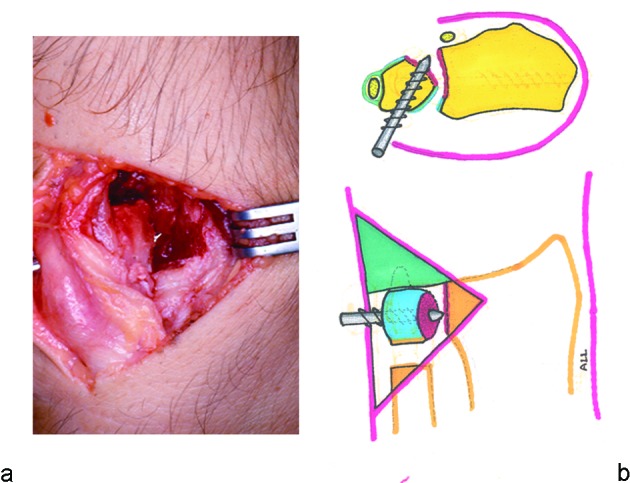
Arthrodesis is the most reliable and durable surgical procedure for the treatment of a joint disorder, and its only disadvantage is the loss of motion of the fused joint. The distal radioulnar joint can be arthrodesed, while forearm pronation and supination are maintained or even improved by creating a pseudoarthrosis of the ulna just proximal to the arthrodesis. This is known as the Sauvé-Kapandji (S-K) procedure. The Sauvé-Kapandji differs from the Darrach procedure in that it preserves ulnar support of the wrist, as the distal radioulnar ligaments and ulnocarpal ligaments are maintained. Aesthetic appearance is also superior after the S-K procedure, as the normal prominence of the ulnar head, most noticeable when the forearm is in pronation, is maintained. However, the S-K is not free of possible complications, such as nonunion or delayed union of the arthrodesis, fibrous or osseous union at the pseudoarthrosis, and painful instability at the proximal ulna stump. All of these complications can be prevented if a careful surgical technique is used.
Keywords: arthrodesis; distal radioulnar joint; triangular fibrocartilage; ulnocarpal impaction.
Conflict of interest statement
Figures

Similar articles
-
The Sauvé-Kapandji procedure: indications and tips for surgical success.Hand Clin. 2010 Nov;26(4):559-72. doi: 10.1016/j.hcl.2010.07.002. Hand Clin. 2010. PMID: 20951905 Review.
-
[Kapandji-Sauvé procedure with distal radioulnar fusion and segmental resection of the ulna].Oper Orthop Traumatol. 2012 Feb;24(1):13-22. doi: 10.1007/s00064-010-8044-7. Oper Orthop Traumatol. 2012. PMID: 20924551 German.
-
Treatment of Proximal Ulnar Stump after Darrach or Sauvé-Kapandji Procedure by Transfer of Insertion-Released Pronator Quadratus Pedicle.J Hand Surg Asian Pac Vol. 2021 Mar;26(1):70-76. doi: 10.1142/S2424835521500119. J Hand Surg Asian Pac Vol. 2021. PMID: 33559564
-
Treatments of osteoarthritis of the distal radioulnar joint: long-term results of three procedures.Hand Surg. 2005;10(2-3):243-8. doi: 10.1142/S0218810405002942. Hand Surg. 2005. PMID: 16568521
-
[Clinical application progress of the Sauvé-Kapandji procedure].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2017 Sep 15;31(9):1131-1134. doi: 10.7507/1002-1892.201702087. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2017. PMID: 29798574 Free PMC article. Review. Chinese.
Cited by
-
Ossification of the pseudarthrosis following the Sauvé-Kapandji procedure: a case report and review of the literature.Case Reports Plast Surg Hand Surg. 2021 Apr 16;8(1):66-71. doi: 10.1080/23320885.2021.1910040. Case Reports Plast Surg Hand Surg. 2021. PMID: 33997111 Free PMC article.
-
Extensor Tendon Rupture After Distal Radioulnar Joint Surgery: A Case Series.Cureus. 2021 Mar 25;13(3):e14118. doi: 10.7759/cureus.14118. Cureus. 2021. PMID: 33927927 Free PMC article.
-
Functional outcomes after the Sauvé-Kapandji procedure for distal radio-ulnar post-traumatic instability: a case-control comparison of three different operative methods of stabilization of the ulnar stump.Int Orthop. 2018 Sep;42(9):2173-2179. doi: 10.1007/s00264-018-4042-4. Epub 2018 Jun 29. Int Orthop. 2018. PMID: 29955946
-
Assessment of Distal Radioulnar Joint Stability After Reconstruction With the Brachioradialis Wrap.Hand (N Y). 2018 Jul;13(4):455-460. doi: 10.1177/1558944717708026. Epub 2017 May 26. Hand (N Y). 2018. PMID: 28549397 Free PMC article.
-
Treatment Outcomes in Patients Undergoing Surgical Treatment for Arthritis of the Distal Radioulnar Joint.J Wrist Surg. 2020 Jun;9(3):230-234. doi: 10.1055/s-0040-1702200. Epub 2020 Mar 16. J Wrist Surg. 2020. PMID: 32509428 Free PMC article.
References
-
- Lichtman D M, Ganocy T K, Kim D C. The indications for and techniques and outcomes of ablative procedures of the distal ulna. The Darrach resection, hemiresection, matched resection, and Sauvé-Kapandji procedure. Hand Clin . 1998;14(2):265–277. - PubMed
-
- Malgaine J F. Paris: JB Braillière; 1855. Traité des fractures et des luxations. Vol 2.
-
- Darrach W. Anterior dislocation of the head of the ulna. Ann Surg. 1912;56:802–803.
-
- Darrach W. Partial excision of lower shaft of the ulna for deformity following Colles's fracture. Ann. Surg . 1913;57:764–765. - PubMed
-
- Baldwin W I. London, England: Henry Frowde and Hodder & Stoughton; 1921. Orthopaedic surgery of the hand and wrist; pp. 241–282.
LinkOut - more resources
Full Text Sources
Other Literature Sources
