

Endoscopic management of cerebrospinal fluid rhinorrhea: the charing cross experience
- PMID: 24436890
- PMCID: PMC3699213
- DOI: 10.1055/s-0033-1333620
Endoscopic management of cerebrospinal fluid rhinorrhea: the charing cross experience
Abstract
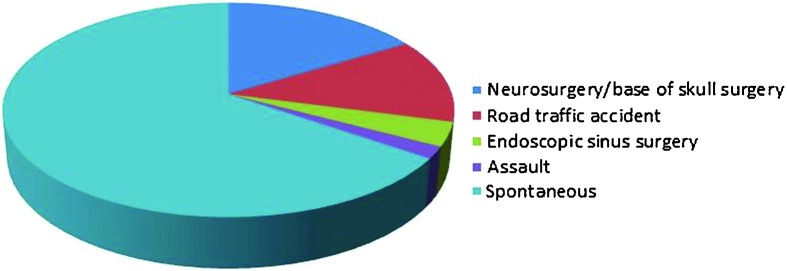
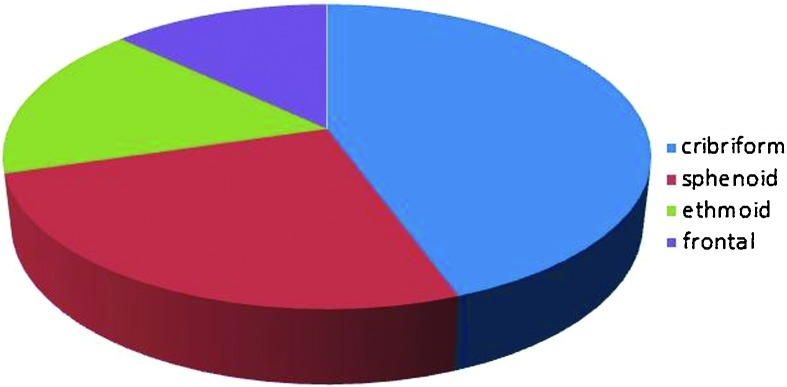
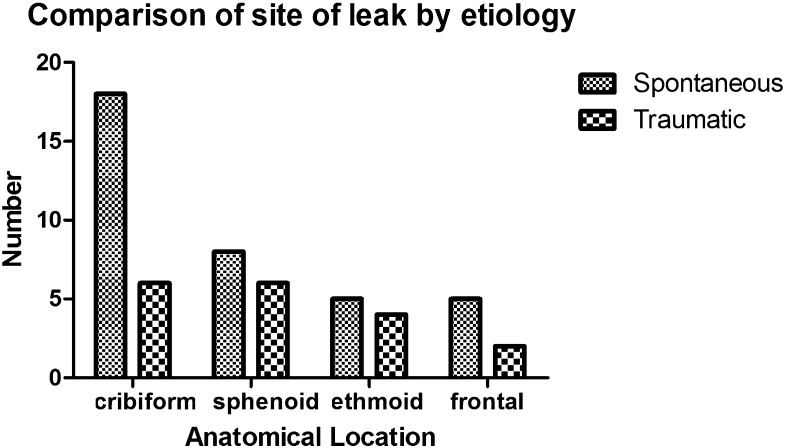
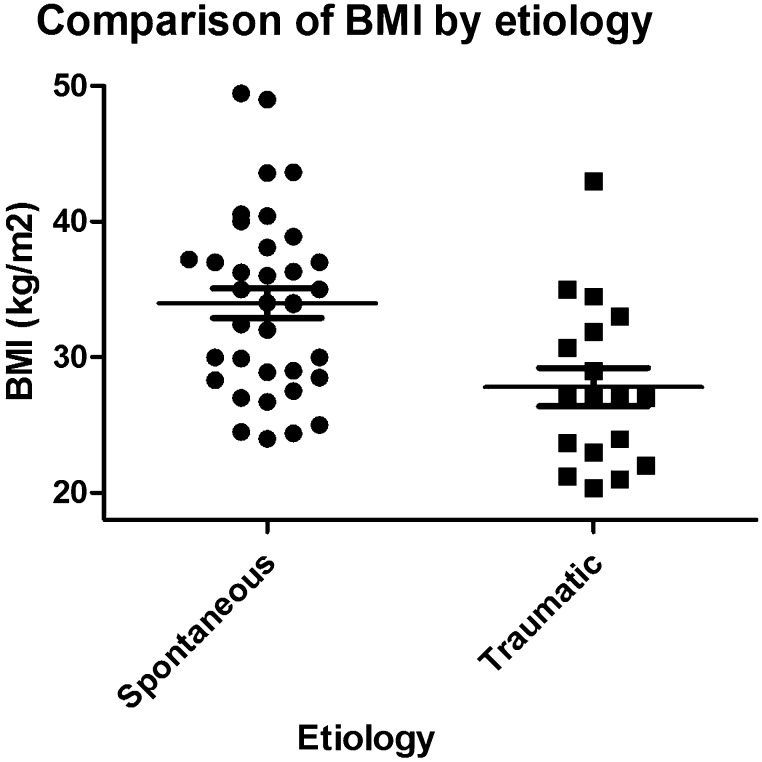
Objective To describe our experience of cerebrospinal fluid (CSF) rhinorrhea management. Design Retrospective. Setting Charing Cross Hospital, London, a tertiary referral center. Participants Fifty-four patients with CSF rhinorrhea managed from 2003 to 2011. Main outcome measures Surgical technique; Recurrence. Results Etiologically, 36 were spontaneous and 18 traumatic. Eight patients with spontaneous and two with traumatic leaks had previous failed repairs in other units. Success rates after first and second surgery were 93% and 100%, respectively. Mean follow-up was 21 months. Four patients, all of spontaneous etiology, had recurrences; three of these underwent successful second repair with three layered technique, and the fourth had complete cessation of the leak after gastric bypass surgery and subsequent weight reduction. Adaptation of anatomic three-layered repair since then averted any further failure in the following 7 years. Mean body mass index was 34.0 kg/m(2) in spontaneous and 27.8 kg/m(2) in traumatic cases (p < 0.05). Fifty percent of spontaneous leaks were from the cribriform plate, 22% sphenoid, 14% ethmoid, and 14% frontal sinus. In the traumatic CSF leak group: 33.3% were from the cribriform plate, 33.3% sphenoid, 22.2% ethmoid, and 11.1% frontal. Conclusion Endoscopic CSF fistula closure is a safe and effective operation. All sites of leak can be accessed endoscopically. We recommend the use of an anatomic three-layered closure in difficult cases.
Keywords: cerebrospinal fluid; endoscopic; rhinorrhea; skull base; spontaneous leaks.
Conflict of interest statement
Figures
Similar articles
-
Optimising outcomes in the management of spontaneous cerebrospinal fluid rhinorrhoea.Rhinology. 2013 Sep;51(3):268-74. doi: 10.4193/Rhino13.008. Rhinology. 2013. PMID: 23943736
-
The Endonasal Endoscopic Management of Cerebrospinal Fluid Rhinorrhea.Cureus. 2021 Feb 20;13(2):e13457. doi: 10.7759/cureus.13457. Cureus. 2021. PMID: 33777546 Free PMC article.
-
The "Parachute" Technique for the Endoscopic Repair of High-Flow Anterior Skull-Base CSF Leaks.World Neurosurg. 2021 Jul;151:e880-e887. doi: 10.1016/j.wneu.2021.05.006. Epub 2021 May 8. World Neurosurg. 2021. PMID: 33974988
-
Endoscopic management of cerebrospinal fluid rhinorrhea.Asian J Neurosurg. 2016 Jul-Sep;11(3):183-93. doi: 10.4103/1793-5482.145101. Asian J Neurosurg. 2016. PMID: 27366243 Free PMC article. Review.
-
Endoscopic repair of cerebrospinal fluid rhinorrhoea.Eur Ann Otorhinolaryngol Head Neck Dis. 2016 Jun;133(3):187-90. doi: 10.1016/j.anorl.2015.05.010. Epub 2016 Jan 6. Eur Ann Otorhinolaryngol Head Neck Dis. 2016. PMID: 26776882 Review.
Cited by
-
Management of Spontaneous CSF Rhinorrhea: An Institutional Experience.J Neurol Surg B Skull Base. 2019 Oct;80(5):493-499. doi: 10.1055/s-0038-1676334. Epub 2018 Dec 5. J Neurol Surg B Skull Base. 2019. PMID: 31534891 Free PMC article.
-
Chemotherapy associated dural sinus thrombosis presenting as a cerebrospinal fluid leak.BMJ Case Rep. 2020 Jun 1;13(6):e235240. doi: 10.1136/bcr-2020-235240. BMJ Case Rep. 2020. PMID: 32487533 Free PMC article.
-
Spontaneous cerebrospinal fluid leak at the clivus.Wideochir Inne Tech Maloinwazyjne. 2016 Jan;10(4):593-9. doi: 10.5114/wiitm.2015.55676. Epub 2015 Nov 20. Wideochir Inne Tech Maloinwazyjne. 2016. PMID: 26865899 Free PMC article.
-
Surgical repair of spontaneous cerebrospinal fluid (CSF) leaks: A systematic review.Laryngoscope Investig Otolaryngol. 2017 Apr 7;2(5):215-224. doi: 10.1002/lio2.75. eCollection 2017 Oct. Laryngoscope Investig Otolaryngol. 2017. PMID: 29094066 Free PMC article. Review.
-
Trans-Nasal Endoscopic Repair of CSF Rhinorrhea: An Institutional Experience.Indian J Otolaryngol Head Neck Surg. 2024 Feb;76(1):748-752. doi: 10.1007/s12070-023-04267-2. Epub 2023 Oct 13. Indian J Otolaryngol Head Neck Surg. 2024. PMID: 38440577 Free PMC article.
References
-
- Locatelli D Rampa F Acchiardi I Bignami M De Bernardi F Castelnuovo P Endoscopic endonasal approaches for repair of cerebrospinal fluid leaks: nine-year experience Neurosurgery 200658402ONS-246–ONS-256., discussion ONS-256–ONS-257 - PubMed
-
- Carrau R L, Snyderman C H, Kassam A B. The management of cerebrospinal fluid leaks in patients at risk for high-pressure hydrocephalus. Laryngoscope. 2005;115:205–212. - PubMed
-
- Har-El G. What is “spontaneous” cerebrospinal fluid rhinorrhea? Classification of cerebrospinal fluid leaks. Ann Otol Rhinol Laryngol. 1999;108:323–326. - PubMed
-
- Wang E W, Vandergrift W A III, Schlosser R J. Spontaneous CSF leaks. Otolaryngol Clin North Am. 2011;44:845–856, vii. - PubMed
-
- Daudia A, Biswas D, Jones N S. Risk of meningitis with cerebrospinal fluid rhinorrhea. Ann Otol Rhinol Laryngol. 2007;116:902–905. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
