

Cerebrospinal Fluid Leakage from Tegmen Tympani Defects Repaired via the Middle Cranial Fossa Approach
- PMID: 24436896
- PMCID: PMC3699214
- DOI: 10.1055/s-0033-1333616
Cerebrospinal Fluid Leakage from Tegmen Tympani Defects Repaired via the Middle Cranial Fossa Approach
Abstract
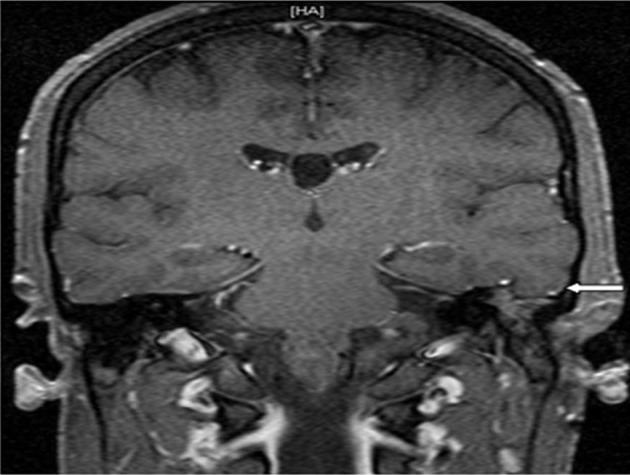
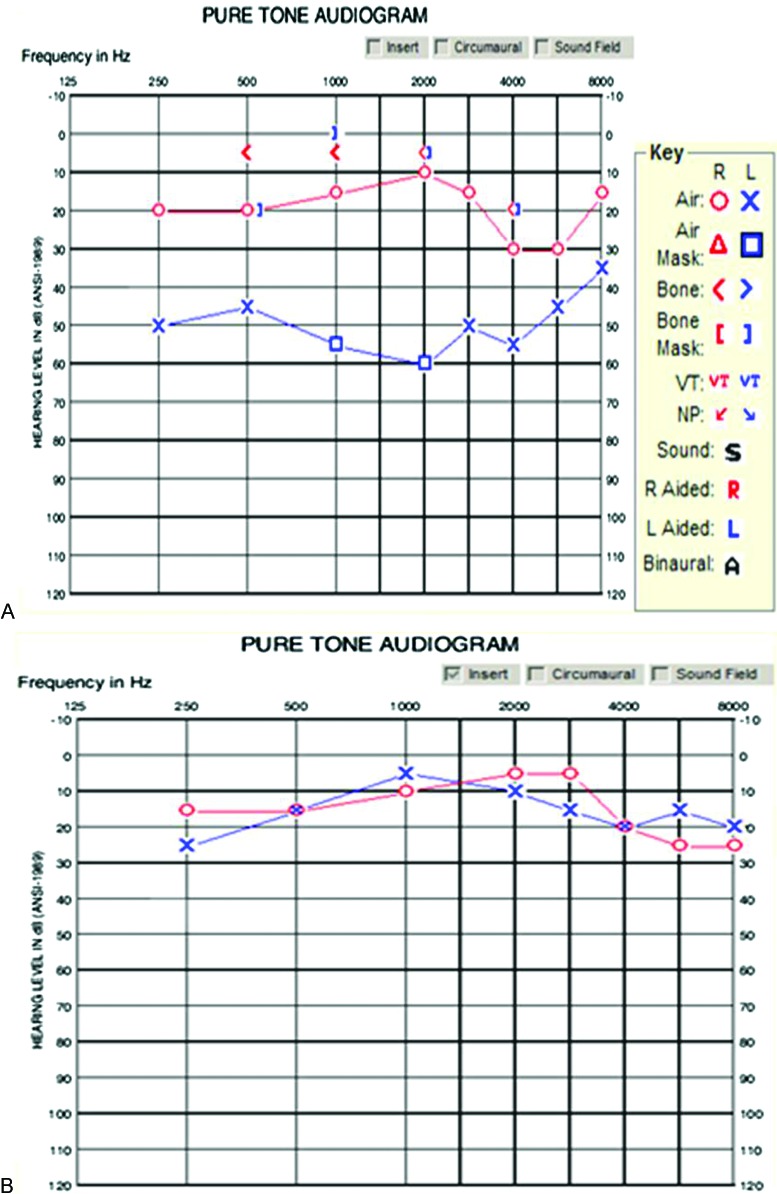
Spontaneous cerebrospinal fluid (CSF) otorrhea due to tegmen tympani defects can result in hearing impairment and predispose to meningitis. Seizures or neurological deficits are additional risks, particularly when associated with an encephalocele. Surgical repair of the dural defect through a middle cranial fossa (MCF) approach is a treatment option under these circumstances. This series describes eight individuals who presented with CSF otorrhea and MCF encephaloceles associated with conductive hearing loss. Defects in the tegmen tympani were noted in all patients on preoperative cranial imaging, and six of the eight patients had an associated encephalocele. The average age was 57 years (range 26 to 67) with a male:female ratio of 7:1. Most defects occurred on the left side (6 left/2 right). A standard MCF approach and repair of the dural defect with an autologous dural graft (Durepair or DuraGen, Medtronic, Minneapolis, Minnesota, USA) and a synthetic polymer glue (DuraSeal, Covidien, Mansfield, Massachusetts) was performed in each case with universal success. Resolution of the CSF otorrhea was noted in all cases. All cases but one exhibited an improvement in hearing. One patient developed a delayed methicillin-resistant Staphylococcus aureus meningitis 3 months after surgery that resolved with surgical re-exploration and antibiotic therapy. Facial nerve monitoring was standard. All patients exhibited normal facial function postoperatively. Prophylactic lumbar drain placement was only utilized in the first three patients. The MCF approach is an excellent route to effectively repair CSF leaks and encephaloceles due to tegmen tympani and dural defects.
Keywords: cerebrospinal fluid leak; encephalocele; hearing loss; middle cranial fossa; otorrhea; tegmen tympani.
Figures
References
-
- Lang D V. Macroscopic bony deficiency of the tegmen tympani in adult temporal bones. J Laryngol Otol. 1983;97:685–688. - PubMed
-
- Parisier S C The middle cranial fossa approach to the internal auditory canal: An anatomic study stressing critical distances between surgical landmarks Laryngosope 197787(suppl):1–20. - PubMed
-
- Kadri P A, Al-Mefty O. The anatomical basis for surgical preservation of temporal muscle. J Neurosurg. 2004;100:517–522. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
