

Response of an aggressive periosteal aneurysmal bone cyst (ABC) of the radius to denosumab therapy
- PMID: 24438319
- PMCID: PMC3901337
- DOI: 10.1186/1477-7819-12-17
Response of an aggressive periosteal aneurysmal bone cyst (ABC) of the radius to denosumab therapy
Abstract
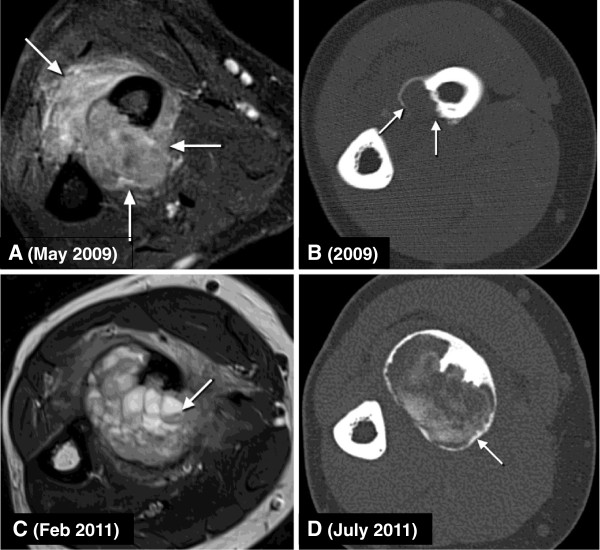
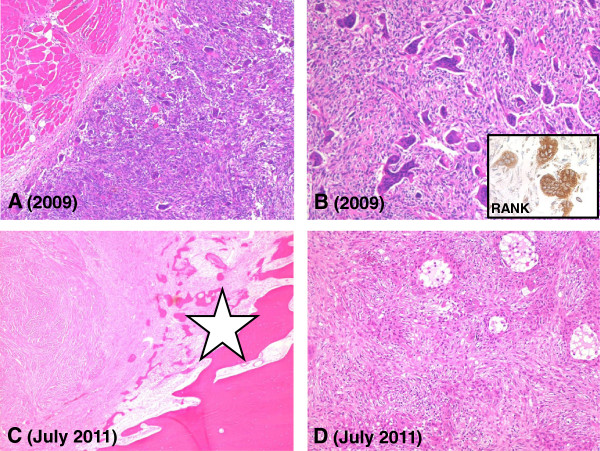
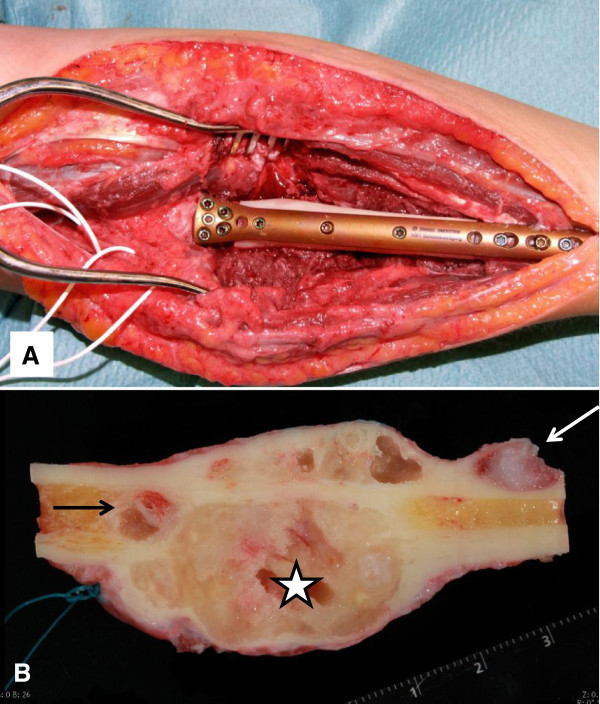
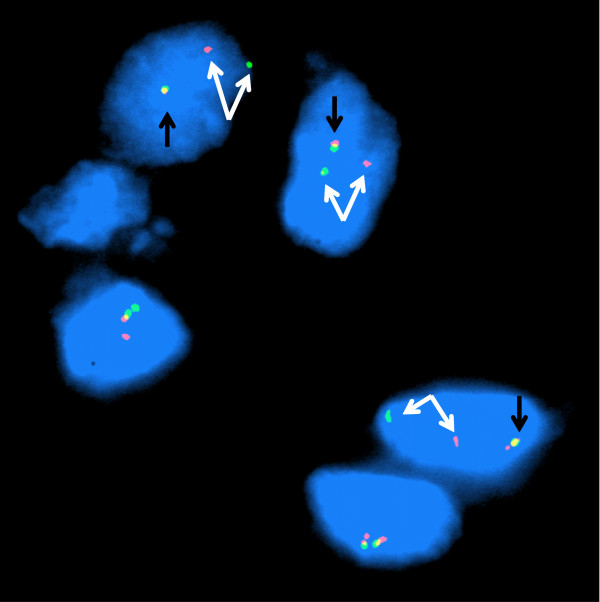
Aneurysmal bone cyst (ABC), once considered a reactive lesion, has been proven to be a neoplasia characterized by rearrangements of the USP6-gene. Aggressive local growth and recurrences are common and therapeutic options may be limited due to the vicinity of crucial structures. We describe a case of a locally aggressive, multinucleated giant cell-containing lesion of the forearm of a 21-year old woman, treated with denosumab for recurrent, surgically uncontrollable disease. Under the influence of this RANKL inhibitor, the tumor showed a marked reduction of the content of the osteoclastic giant cells and an extensive metaplastic osteoid production leading to the bony containment, mostly located intracortically in the proximal radius. The diagnosis of a periosteal ABC was confirmed by FISH demonstrating USP6 gene rearrangement on the initial biopsy. Function conserving surgery could be performed, enabling reconstruction of the affected bone. Inhibition of RANKL with denosumab may offer therapeutic option for patients not only with giant cell tumors but also with ABCs.
Figures
References
-
- Campanacci M, Cervellati C, Donati U, Bertoni F. Aneurysmal bone cyst (a study of 127 cases, 72 with long term follow up) Ital J Orthop Traumatol. 1976;2:341–353. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
