

Obesity paradox in end-stage kidney disease patients
- PMID: 24438733
- PMCID: PMC4733536
- DOI: 10.1016/j.pcad.2013.10.005
Obesity paradox in end-stage kidney disease patients
Abstract
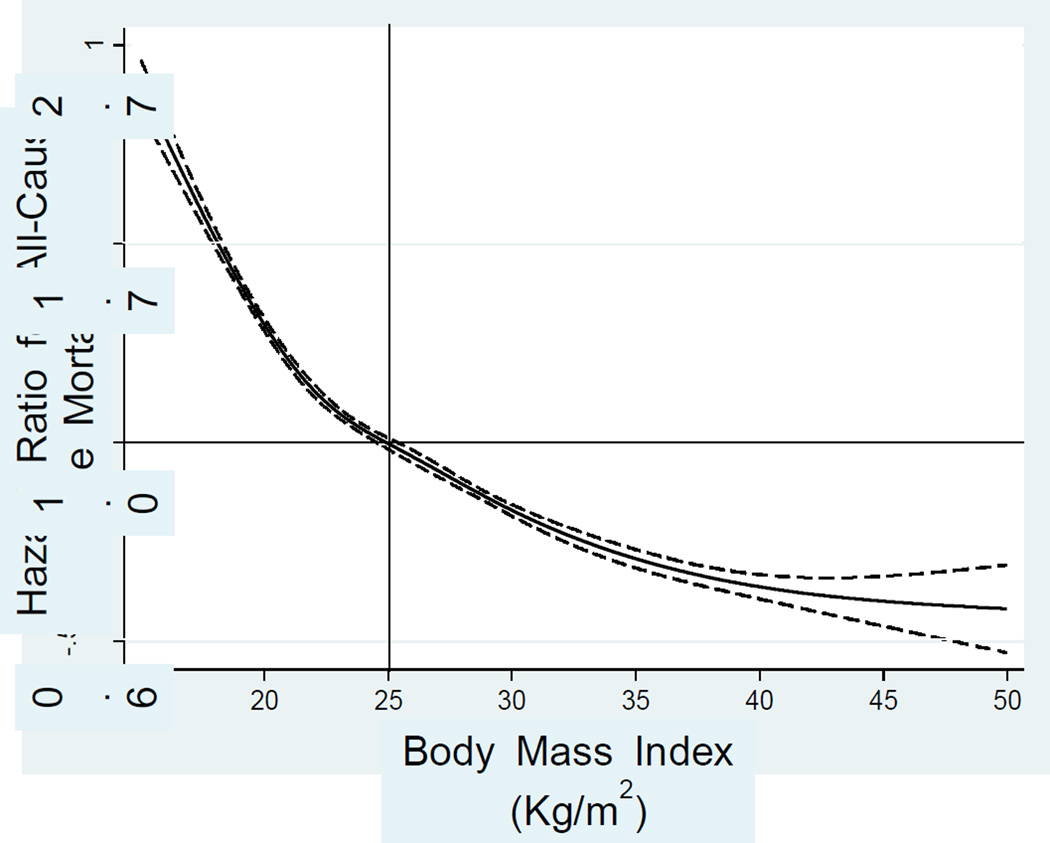
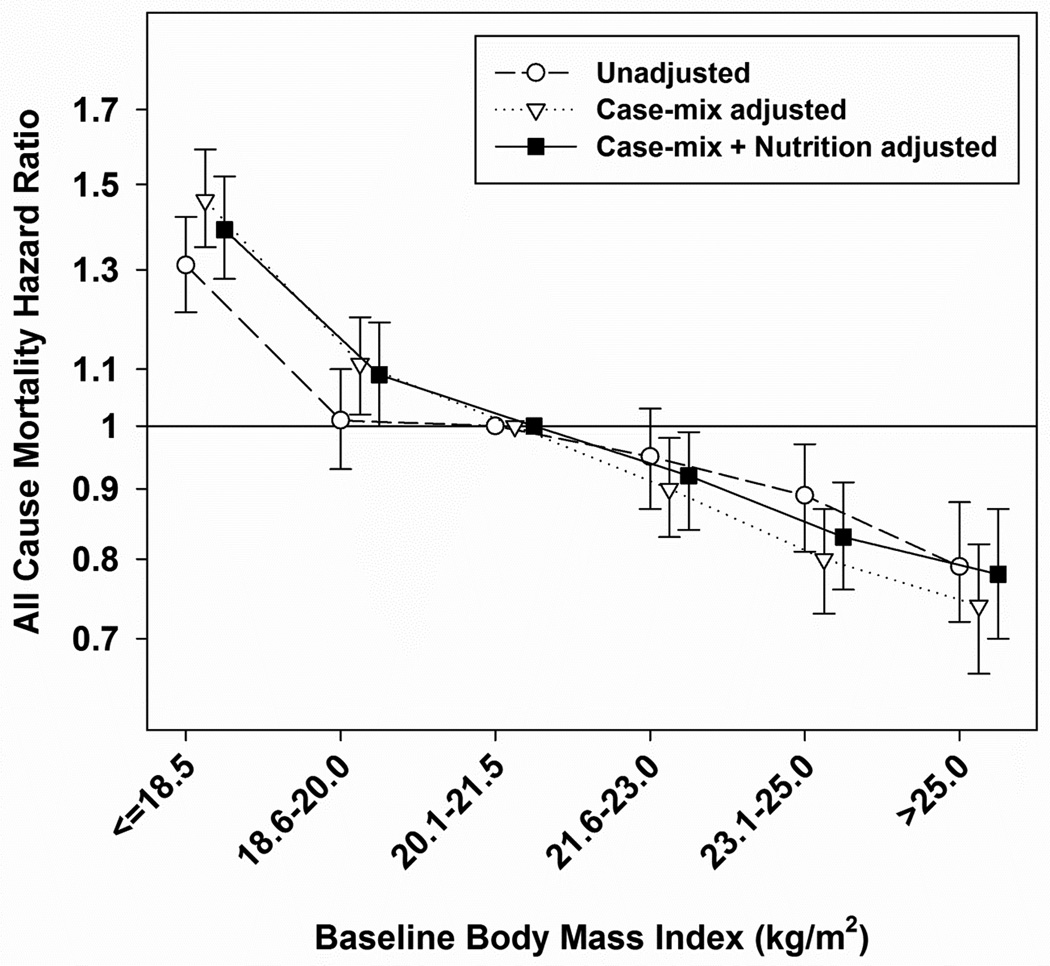
In the general population, obesity is associated with increased cardiovascular risk and decreased survival. In patients with end-stage renal disease (ESRD), however, an "obesity paradox" or "reverse epidemiology" (to include lipid and hypertension paradoxes) has been consistently reported, i.e. a higher body mass index (BMI) is paradoxically associated with better survival. This survival advantage of large body size is relatively consistent for hemodialysis patients across racial and regional differences, although published results are mixed for peritoneal dialysis patients. Recent data indicate that both higher skeletal muscle mass and increased total body fat are protective, although there are mixed data on visceral (intra-abdominal) fat. The obesity paradox in ESRD is unlikely to be due to residual confounding alone and has biologic plausibility. Possible causes of the obesity paradox include protein-energy wasting and inflammation, time discrepancy among competitive risk factors (undernutrition versus overnutrition), hemodynamic stability, alteration of circulatory cytokines, sequestration of uremic toxin in adipose tissue, and endotoxin-lipoprotein interaction. The obesity paradox may have significant clinical implications in the management of ESRD patients especially if obese dialysis patients are forced to lose weight upon transplant wait-listing. Well-designed studies exploring the causes and consequences of the reverse epidemiology of cardiovascular risk factors, including the obesity paradox, among ESRD patients could provide more information on mechanisms. These could include controlled trials of nutritional and pharmacologic interventions to examine whether gain in lean body mass or even body fat can improve survival and quality of life in these patients.
Keywords: BMI; CKD; CVD; Dialysis; ESRD; HD; Obesity paradox; PD; PEW; Reverse epidemiology; Visceral fat; body mass index; cardiovascular diseases; chronic kidney disease; end-stage renal disease; hemodialysis; peritoneal dialysis; protein energy wasting.
© 2014.
Conflict of interest statement
None declared by the authors.
Figures
References
-
- USRDS 2011 Annual Data Report: Atlas of End-Stage Renal Disease in the United States. [Accessed July 1, 2013]; http://www.usrds.org/atlas.asps.
-
- Goodkin DA, Mapes DL, Held PJ. The dialysis outcomes and practice patterns study (DOPPS): how can we improve the care of hemodialysis patients? Semin Dial. 2001;14(3):157–159. - PubMed
-
- Besarab A, et al. The effects of normal as compared with low hematocrit values in patients with cardiac disease who are receiving hemodialysis and epoetin. N Engl J Med. 1998;339(9):584–590. - PubMed
-
- Eknoyan G, et al. Effect of dialysis dose and membrane flux in maintenance hemodialysis. N Engl J Med. 2002;347(25):2010–2019. - PubMed
-
- Paniagua R, et al. Effects of increased peritoneal clearances on mortality rates in peritoneal dialysis: ADEMEX, a prospective, randomized, controlled trial. J Am Soc Nephrol. 2002;13(5):1307–1320. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
