

Chemotherapy for isolated locoregional recurrence of breast cancer (CALOR): a randomised trial
- PMID: 24439313
- PMCID: PMC3982874
- DOI: 10.1016/S1470-2045(13)70589-8
Chemotherapy for isolated locoregional recurrence of breast cancer (CALOR): a randomised trial
Abstract
Background: Patients with isolated locoregional recurrences (ILRR) of breast cancer have a high risk of distant metastasis and death from breast cancer. We aimed to establish whether adjuvant chemotherapy improves the outcome of such patients.
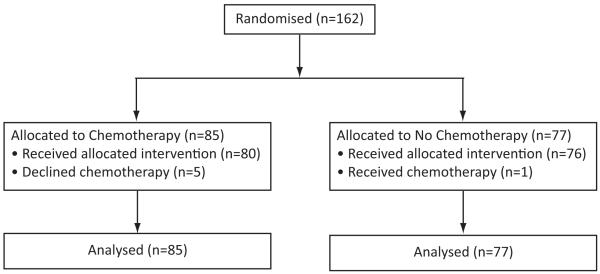
Methods: The CALOR trial was a pragmatic, open-label, randomised trial that accrued patients with histologically proven and completely excised ILRR after unilateral breast cancer who had undergone a mastectomy or lumpectomy with clear surgical margins. Eligible patients were enrolled from hospitals worldwide and were centrally randomised (1:1) to chemotherapy (type selected by the investigator; multidrug for at least four courses recommended) or no chemotherapy, using permuted blocks, and stratified by previous chemotherapy, oestrogen-receptor and progesterone-receptor status, and location of ILRR. Patients with oestrogen-receptor-positive ILRR received adjuvant endocrine therapy, radiation therapy was mandated for patients with microscopically involved surgical margins, and anti-HER2 therapy was optional. The primary endpoint was disease-free survival. All analyses were by intention to treat. This study is registered with ClinicalTrials.gov, number NCT00074152.
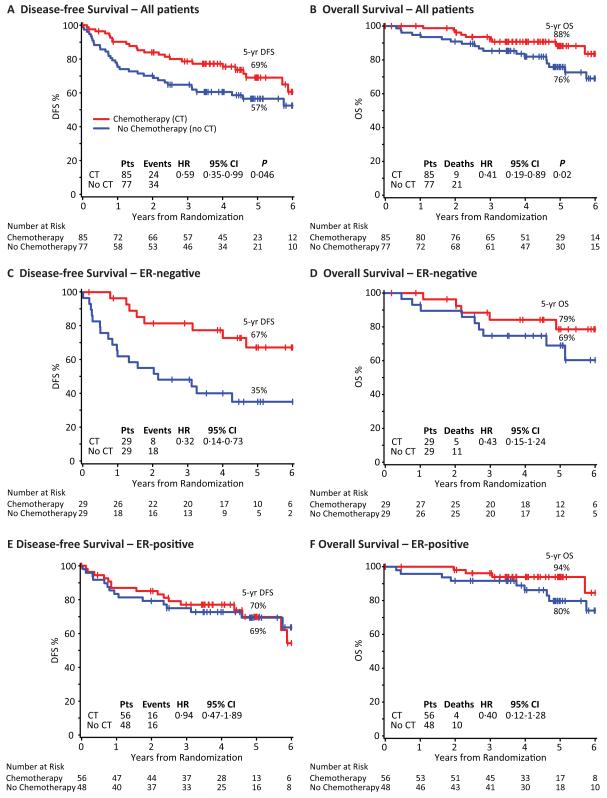
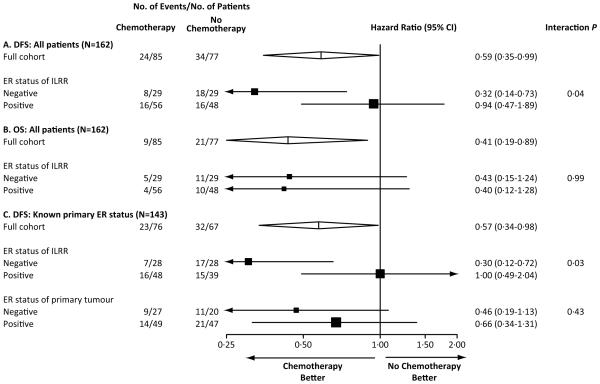
Findings: From Aug 22, 2003, to Jan 31, 2010, 85 patients were randomly assigned to receive chemotherapy and 77 were assigned to no chemotherapy. At a median follow-up of 4·9 years (IQR 3·6-6 ·0), 24 (28%) patients had disease-free survival events in the chemotherapy group compared with 34 (44%) in the no chemotherapy group. 5-year disease-free survival was 69% (95% CI 56-79) with chemotherapy versus 57% (44-67) without chemotherapy (hazard ratio 0·59 [95% CI 0·35-0·99]; p=0·046). Adjuvant chemotherapy was significantly more effective for women with oestrogen-receptor-negative ILRR (pinteraction=0·046), but analyses of disease-free survival according to the oestrogen-receptor status of the primary tumour were not statistically significant (pinteraction=0·43). Of the 81 patients who received chemotherapy, 12 (15%) had serious adverse events. The most common adverse events were neutropenia, febrile neutropenia, and intestinal infection.
Interpretation: Adjuvant chemotherapy should be recommended for patients with completely resected ILRR of breast cancer, especially if the recurrence is oestrogen-receptor negative.
Funding: US Department of Health and Human Services, Swiss Group for Clinical Cancer Research (SAKK), Frontier Science and Technology Research Foundation, Australian and New Zealand Breast Cancer Trials Group, Swedish Cancer Society, Oncosuisse, Cancer Association of South Africa, Foundation for Clinical Research of Eastern Switzerland (OSKK), Grupo Español de Investigación en Cáncer de Mama (GEICAM), and the Dutch Breast Cancer Trialists' Group (BOOG).
Copyright © 2014 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Adjuvant chemotherapy for local relapse breast cancer.Lancet Oncol. 2014 Feb;15(2):125-6. doi: 10.1016/S1470-2045(13)70610-7. Epub 2014 Jan 16. Lancet Oncol. 2014. PMID: 24439312 No abstract available.
-
Breast cancer: CALOR favours adjuvant therapy for ILRR of breast cancer.Nat Rev Clin Oncol. 2014 Mar;11(3):120. doi: 10.1038/nrclinonc.2014.13. Epub 2014 Feb 4. Nat Rev Clin Oncol. 2014. PMID: 24492831 No abstract available.
References
-
- Clemons M, Danson S, Hamilton T, Goss P. Locoregionally recurrent breast cancer: incidence, risk factors and survival. Cancer Treat Rev. 2001;27:67–82. - PubMed
-
- Haffty BG, Fischer D, Beinfield M, McKhann C. Prognosis following local recurrence in the conservatively treated breast cancer patient. Int J Radiat Oncol Biol Phys. 1991;21:293–8. - PubMed
-
- Abner AL, Recht A, Eberlein T, et al. Prognosis following salvage mastectomy for recurrence in the breast after conservative surgery and radiation therapy for early-stage breast cancer. J Clin Oncol. 1993;11:44–8. - PubMed
-
- Whelan T, Clark R, Roberts R, Levine M, Foster G. Ipsilateral breast tumor recurrence postlumpectomy is predictive of subsequent mortality: results from a randomized trial. Investigators of the Ontario Clinical Oncology Group. Int J Radiat Oncol Biol Phys. 1994;30:11–6. - PubMed
-
- Haffty BG, Reiss M, Beinfield M, Fischer D, Ward B, McKhann C. Ipsilateral breast tumor recurrence as a predictor of distant disease: implications for systemic therapy at the time of local relapse. J Clin Oncol. 1996;14:52–7. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
