

Systemic oxygen delivery by peritoneal perfusion of oxygen microbubbles
- PMID: 24439406
- PMCID: PMC7124456
- DOI: 10.1016/j.biomaterials.2013.12.070
Systemic oxygen delivery by peritoneal perfusion of oxygen microbubbles
Abstract
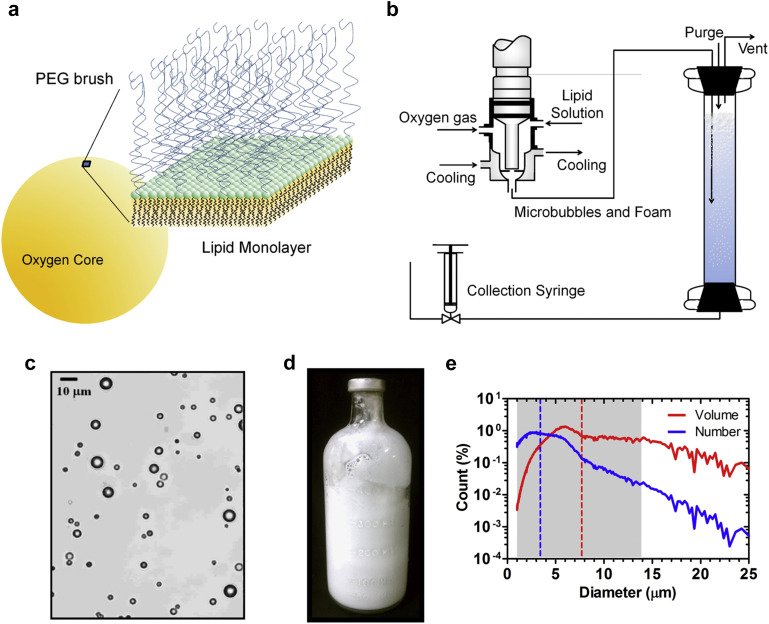
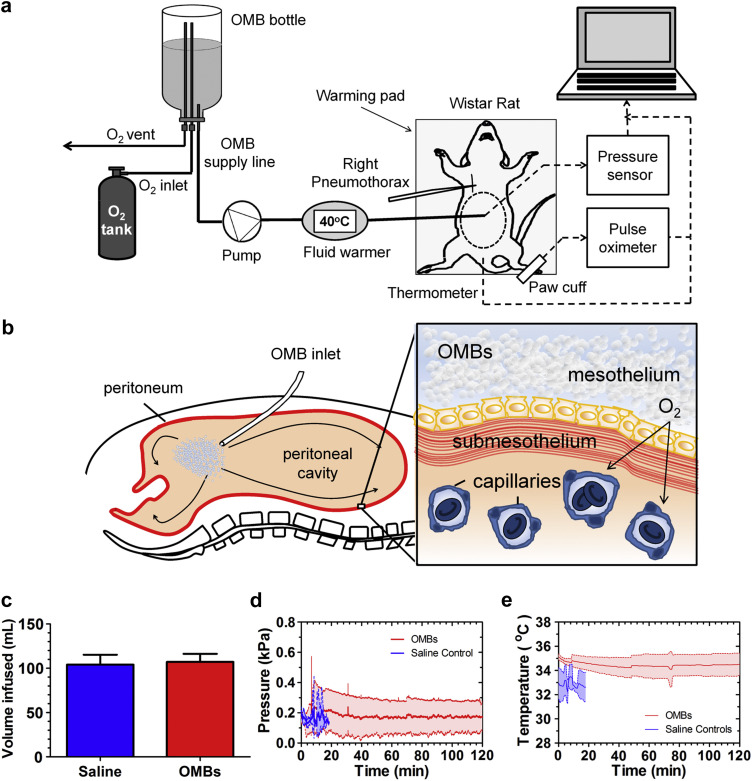
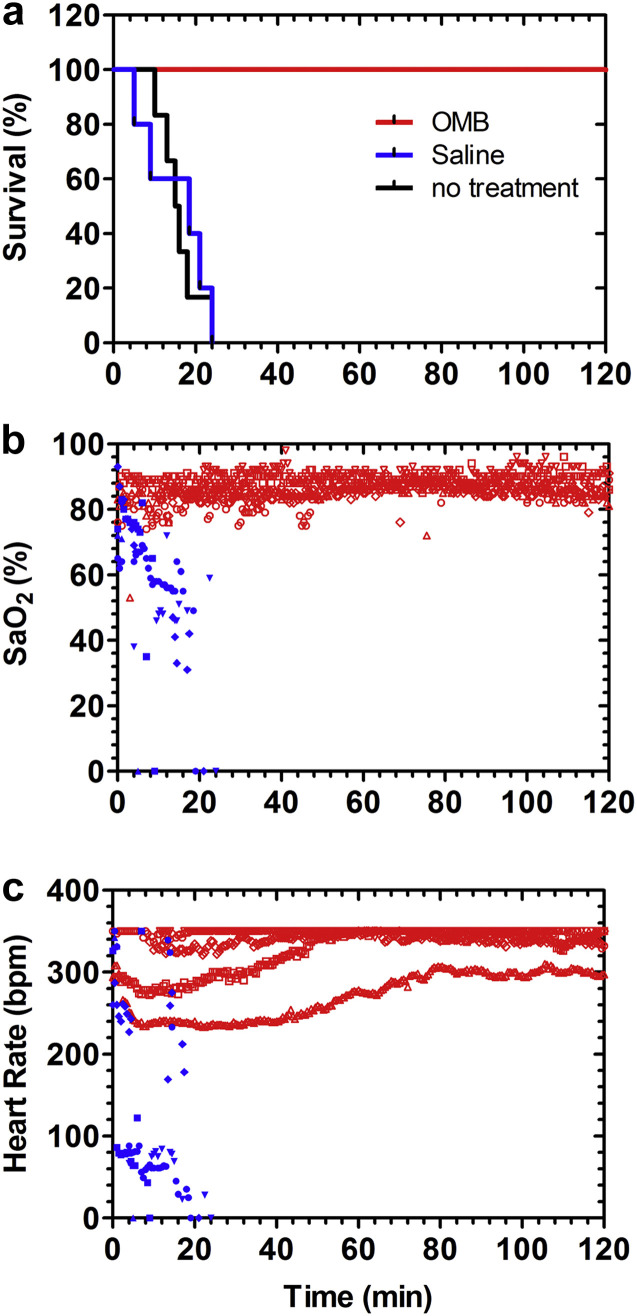
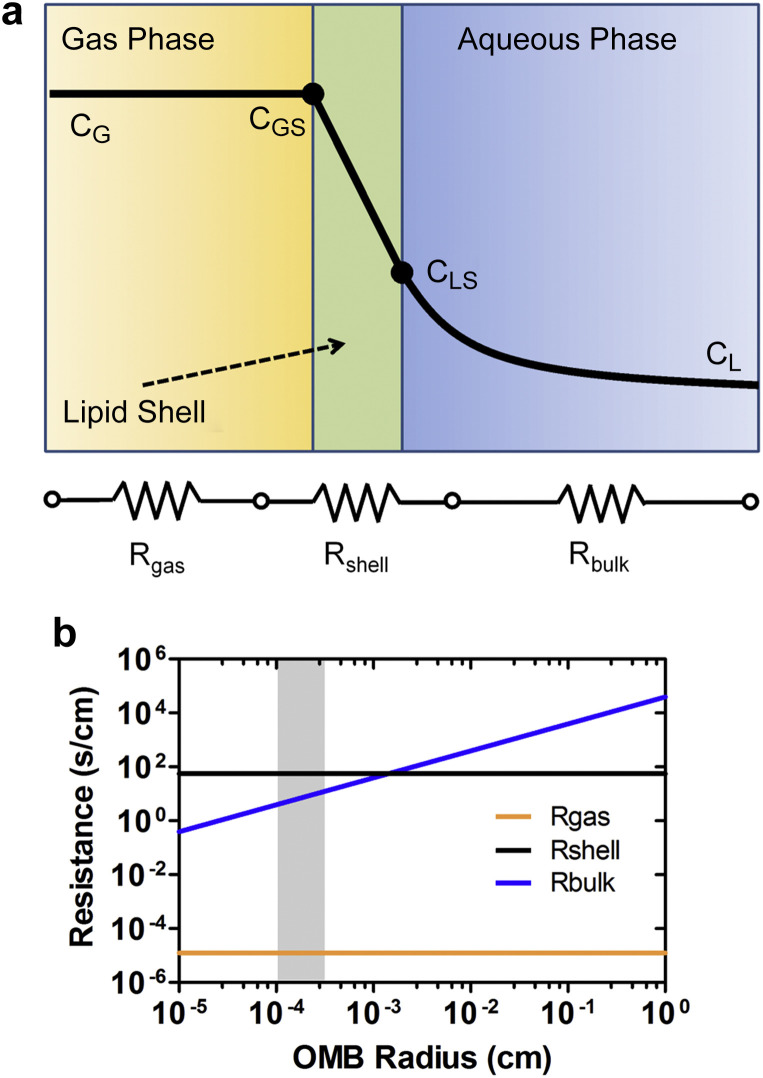
Severe hypoxemia refractory to pulmonary mechanical ventilation remains life-threatening in critically ill patients. Peritoneal ventilation has long been desired for extrapulmonary oxygenation owing to easy access of the peritoneal cavity for catheterization and the relative safety compared to an extracorporeal circuit. Unfortunately, prior attempts involving direct oxygen ventilation or aqueous perfusates of fluorocarbons or hemoglobin carriers have failed, leading many researchers to abandon the method. We attribute these prior failures to limited mass transfer of oxygen to the peritoneum and have designed an oxygen formulation that overcomes this limitation. Using phospholipid-coated oxygen microbubbles (OMBs), we demonstrate 100% survival for rats experiencing acute lung trauma to at least 2 h. In contrast, all untreated rats and rats treated with peritoneal oxygenated saline died within 30 min. For rats treated with OMBs, hemoglobin saturation and heart rate were at normal levels over the 2-h timeframe. Peritoneal oxygenation with OMBs was therefore shown to be safe and effective, and the method requires less equipment and technical expertise than initiating and maintaining an extracorporeal circuit. Further translation of peritoneal oxygenation with OMBs may provide therapy for acute respiratory distress syndrome arising from trauma, sepsis, pneumonia, aspiration, burns and other pulmonary diseases.
Keywords: Acute lung injury; Acute respiratory distress syndrome; Hypoxemia; Oxygen absorption and transport; Phospholipid monolayer.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
Evaluation of peritoneal microbubble oxygenation therapy in a rabbit model of hypoxemia.IEEE Trans Biomed Eng. 2015 May;62(5):1376-82. doi: 10.1109/TBME.2015.2388611. Epub 2015 Jan 6. IEEE Trans Biomed Eng. 2015. PMID: 25576562
-
Peritoneal Oxygenation as a Novel Technique for Extrapulmonary Ventilation; A Review and Discussion of the Literature.Adv Respir Med. 2022 Dec 12;90(6):511-517. doi: 10.3390/arm90060057. Adv Respir Med. 2022. PMID: 36547012 Free PMC article. Review.
-
Treatment of a Rat Model of LPS-Induced ARDS via Peritoneal Perfusion of Oxygen Microbubbles.J Surg Res. 2020 Feb;246:450-456. doi: 10.1016/j.jss.2019.09.017. Epub 2019 Oct 16. J Surg Res. 2020. PMID: 31629496
-
The peritoneum as a novel oxygenation organ: revitalization of intraperitoneal oxygenation.Shock. 2008 Sep;30(3):250-3. doi: 10.1097/shk.0b013e318162be0a. Shock. 2008. PMID: 18197147
-
Ventilator strategies for posttraumatic acute respiratory distress syndrome: airway pressure release ventilation and the role of spontaneous breathing in critically ill patients.Curr Opin Crit Care. 2004 Dec;10(6):549-57. doi: 10.1097/01.ccx.0000145473.01597.13. Curr Opin Crit Care. 2004. PMID: 15616399 Review.
Cited by
-
Development of quantitative and concise measurement method of oxygen in fine bubble dispersion.PLoS One. 2022 Feb 16;17(2):e0264083. doi: 10.1371/journal.pone.0264083. eCollection 2022. PLoS One. 2022. PMID: 35171962 Free PMC article.
-
Reducing Tumour Hypoxia via Oral Administration of Oxygen Nanobubbles.PLoS One. 2016 Dec 30;11(12):e0168088. doi: 10.1371/journal.pone.0168088. eCollection 2016. PLoS One. 2016. PMID: 28036332 Free PMC article.
-
Reverse engineering the ultrasound contrast agent.Adv Colloid Interface Sci. 2018 Dec;262:39-49. doi: 10.1016/j.cis.2018.10.004. Epub 2018 Oct 24. Adv Colloid Interface Sci. 2018. PMID: 30396507 Free PMC article. Review.
-
Magnetic resonance imaging of oxygen microbubbles.Healthc Technol Lett. 2019 Aug 21;6(5):138-142. doi: 10.1049/htl.2018.5058. eCollection 2019 Oct. Healthc Technol Lett. 2019. PMID: 31832209 Free PMC article.
-
The Treatment of Acute Respiratory Distress Syndrome in Rats With a Peritoneal Dosing System.J Med Device. 2015 Jun 1;9(2):020929. doi: 10.1115/1.4030140. J Med Device. 2015. PMID: 32328216 Free PMC article. No abstract available.
References
-
- Hill J.D., Bramson M.L., Gerbode F., Osborn J.J., Obrien T.G., Dontigny L. Prolonged extracorporeal oxygenation for acute post-traumatic respiratory failure (shock-lung syndrome) – use of the bramson membrane lung. N Engl J Med. 1972;286:629. - PubMed
-
- Bartlett R.H., Gazzaniga A.B., Jefferies M.R., Huxtable R.F., Haiduc N.J., Fong S.W. Extracorporeal membrane oxygenation (ECMO) cardiopulmonary support in infancy. Tran Am Soc Artif Intern Organs. 1976;22:80–93. - PubMed
-
- Kim E.S., Stolar C.J. ECMO in the newborn. Am J Perinatol. 2000;17:345–356. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
