

A randomized double blind, placebo controlled phase 2 trial of BIIL 284 BS (an LTB4 receptor antagonist) for the treatment of lung disease in children and adults with cystic fibrosis
- PMID: 24440167
- PMCID: PMC4755340
- DOI: 10.1016/j.jcf.2013.12.009
A randomized double blind, placebo controlled phase 2 trial of BIIL 284 BS (an LTB4 receptor antagonist) for the treatment of lung disease in children and adults with cystic fibrosis
Abstract
Background: Airway inflammation, mediated in part by LTB4, contributes to lung destruction in patients with cystic fibrosis (CF). LTB(4)-receptor inhibition may reduce airway inflammation. We report the results of a randomized, double-blind, placebo-controlled study of the efficacy and safety of the leukotriene B(4) (LTB(4))-receptor antagonist BIIL 284 BS in CF patients.
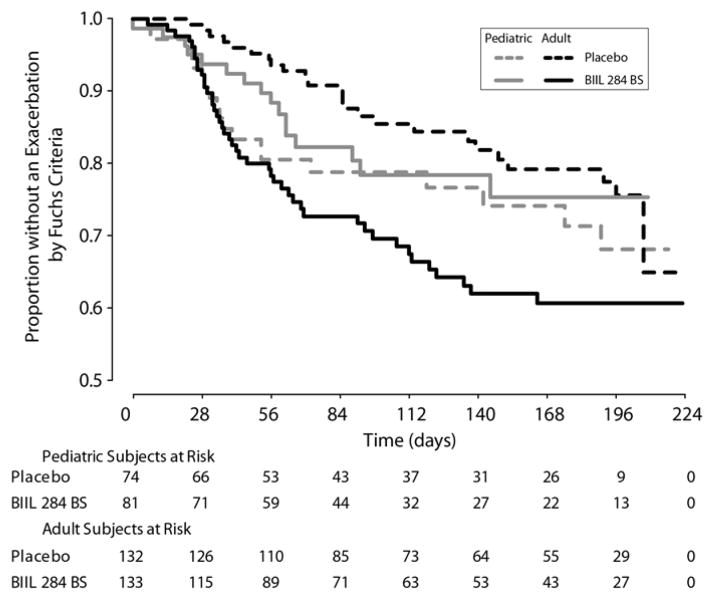
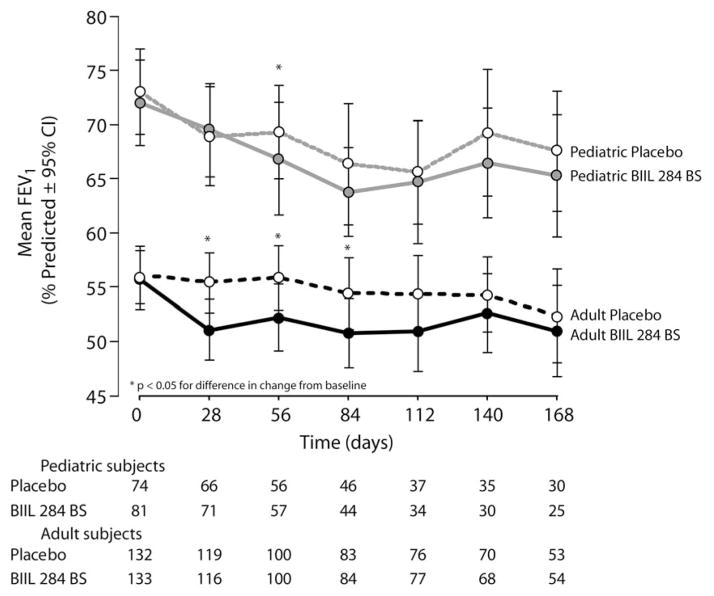
Methods: CF patients aged ≥6 years with mild to moderate lung disease were randomized to oral BIIL 284 BS or placebo once daily for 24 weeks. Co-primary endpoints were change in FEV(1) and incidence of pulmonary exacerbation.
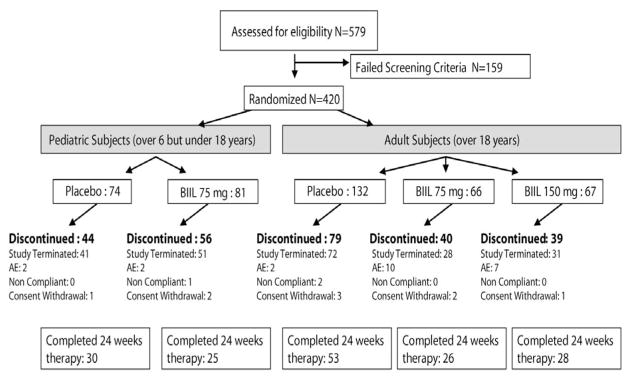
Results: After 420 (155 children, 265 adults) of the planned 600 patients were randomized, the trial was terminated after a planned interim analysis revealed a significant increase in pulmonary related serious adverse events (SAEs) in adults receiving BIIL 284 BS. Final analysis revealed SAEs in 36.1% of adults receiving BIIL 284 BS vs. 21.2% receiving placebo (p = 0.007), and in 29.6% of children receiving BIIL 284 BS vs. 22.9% receiving placebo (p = 0.348). In adults, the incidence of protocol-defined pulmonary exacerbation was greater in those receiving BIIL 284 BS than in those receiving placebo (33.1% vs. 18.2% respectively; p = 0.005). In children, the incidence of protocol-defined pulmonary exacerbation was 19.8% in the BIIL 284 BS arm, and 25.7% in the placebo arm (p = 0.38).
Conclusions: While the cause of increased SAEs and exacerbations due to BIIL 284 BS is unknown, the outcome of this trial provides a cautionary tale for the administration of potent anti-inflammatory compounds to individuals with chronic infections, as the potential to significantly suppress the inflammatory response may increase the risk of infection-related adverse events.
Keywords: Anti-inflammatory therapy; Clinical trial; Cystic fibrosis; Leukotriene B(4) receptor antagonist; Lung disease.
Copyright © 2014 European Cystic Fibrosis Society. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
Clinical Trials of Novel Treatments for Cystic Fibrosis.Am J Respir Crit Care Med. 2016 Mar 1;193(5):569-71. doi: 10.1164/rccm.201509-1734RR. Am J Respir Crit Care Med. 2016. PMID: 26765316 No abstract available.
References
-
- Cantin A. Cystic fibrosis lung inflammation: early, sustained, and severe. Am J Respir Crit Care Med. 1995;151:939–41. - PubMed
-
- Konstan MW, Berger M. Current understanding of the inflammatory process in cystic fibrosis - onset and etiology. Pediatr Pulmonol. 1997;24:137–42. - PubMed
-
- Döring G, Ratjen F. Immunology of cystic fibrosis. In: Hodson ME, Geddes D, Bush A, editors. Cystic Fibrosis. London, England: Arnold Hammer; 2007. pp. 69–80.
-
- Döring G, Conway SP, Heijerman HGM, et al. for the Consensus Committee. Antibiotic therapy against Pseudomonas aeruginosa in cystic fibrosis: a European consensus. Eur Respir J. 2000;16:749–767. - PubMed
-
- Konstan MW. Therapies aimed at airway inflammation in cystic fibrosis. In: Fiel SB, editor. Clinics in Chest Medicine: Cystic Fibrosis. Vol. 19. Philadelphia: W.B, Saunders Co; 1998. pp. 505–513. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
