

Comparative effectiveness of upfront treatment strategies in elderly women with ovarian cancer
- PMID: 24443159
- PMCID: PMC4062652
- DOI: 10.1002/cncr.28508
Comparative effectiveness of upfront treatment strategies in elderly women with ovarian cancer
Abstract
Background: Observational studies comparing neoadjuvant chemotherapy to primary surgery for advanced-stage ovarian cancer are limited by strong selection bias. Multiple methods were used to control for confounding and selection bias to estimate the effect of primary treatment on survival for ovarian cancer.
Methods: The Surveillance, Epidemiology, and End Results (SEER)-Medicare database was used to identify women ≥ 65 years of age with stage II-IV epithelial ovarian cancer who survived > 6 months from the date of diagnosis and received treatment from 1991 through 2007. Traditional regression analysis, propensity score-based analysis, and an instrumental variable analysis (IVA) using geographic location as an instrument were used to compare survival between neoadjuvant chemotherapy and primary surgery.
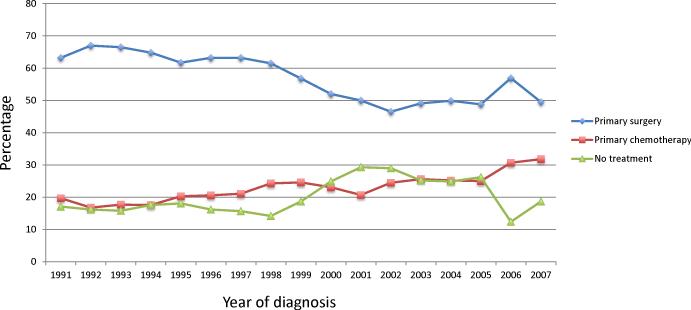
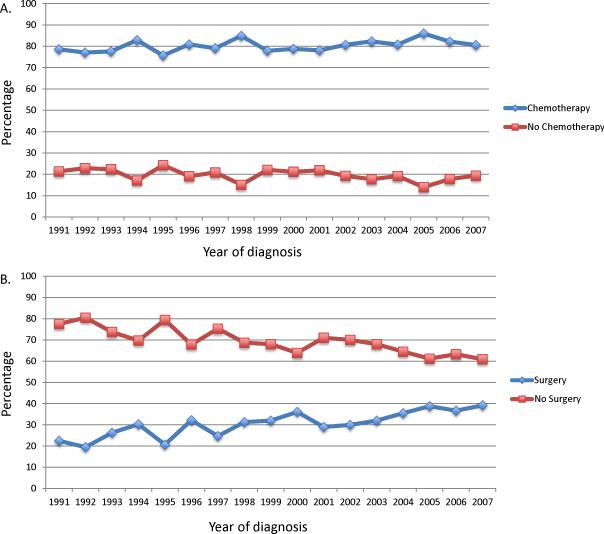
Results: A total of 9587 patients with stage II-IV ovarian cancer were identified. Use of primary surgery decreased from 63.2% in 1991 to 49.5% by 2007, whereas primary chemotherapy increased from 19.7% in 1991 to 31.8% in 2007 (P < .0001). In the observational cohort survival (hazard ratio [HR] = 1.27; 95% confidence interval [CI] = 1.19-1.35) was inferior for patients treated with neoadjuvant chemotherapy; both median survival (15.8 versus 28.8 months) and 2-year survival (36% versus 56%) were lower in the neoadjuvant chemotherapy group compared to those who underwent surgery. In the IVA, primary treatment had minimal effect on overall survival (HR = 1.04; 95% CI = 0.67-1.60). The median survival for patients with a value of the instrument less than the median (24.0 months, 95% CI = 23.0-25.0) and greater than or equal to median value of the IV (24.0 months, 95% CI = 23.0-26.0) were similar.
Conclusions: Use of neoadjuvant therapy has increased over time. Survival with neoadjuvant chemotherapy did not differ significantly from primary surgery in elderly women in the United States.
Keywords: ovarian cancer, cytoreduction, debulking, oophorectomy, chemotherapy.
© 2013 American Cancer Society.
Figures
References
-
- Griffiths CT. Surgical resection of tumor bulk in the primary treatment of ovarian carcinoma. Natl Cancer Inst Monogr. 1975;42:101–4. - PubMed
-
- Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol. 2002;20:1248–59. - PubMed
-
- Vergote I, Trope CG, Amant F, et al. Neoadjuvant chemotherapy or primary surgery in stage IIIC or IV ovarian cancer. N Engl J Med. 2010;363:943–53. - PubMed
-
- Everett EN, French AE, Stone RL, et al. Initial chemotherapy followed by surgical cytoreduction for the treatment of stage III/IV epithelial ovarian cancer. Am J Obstet Gynecol. 2006;195:568–74. discussion 74-6. - PubMed
-
- Bristow RE, Chi DS. Platinum-based neoadjuvant chemotherapy and interval surgical cytoreduction for advanced ovarian cancer: a meta-analysis. Gynecol Oncol. 2006;103:1070–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
