

The potential economic benefits of improved postfracture care: a cost-effectiveness analysis of a fracture liaison service in the US health-care system
- PMID: 24443384
- PMCID: PMC4176766
- DOI: 10.1002/jbmr.2180
The potential economic benefits of improved postfracture care: a cost-effectiveness analysis of a fracture liaison service in the US health-care system
Abstract
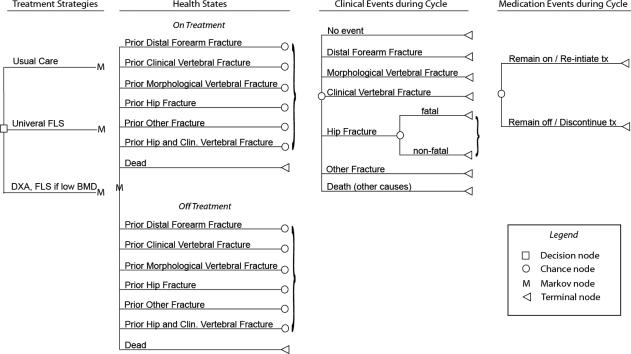
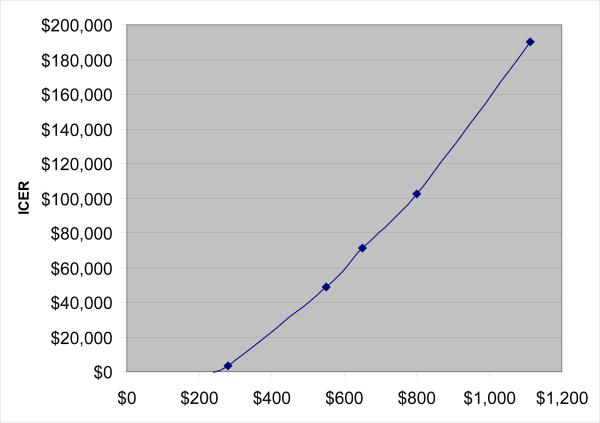
Fractures related to osteoporosis are associated with $20 billion in cost in the United States, with the majority of cost born by federal health-care programs, such as Medicare and Medicaid. Despite the proven fracture reduction benefits of several osteoporosis treatments, less than one-quarter of patients older than 65 years of age who fracture receive such care. A postfracture liaison service (FLS) has been developed in many health systems but has not been widely implemented in the United States. We developed a Markov state-transition computer simulation model to assess the cost-effectiveness of an FLS using a health-care system perspective. Using the model, we projected the lifetime costs and benefits of FLS, with or without a bone mineral density test, in men and women who had experienced a hip fracture. We estimated the costs and benefits of an FLS, the probabilities of refracture while on osteoporosis treatment, as well as the utilities associated with various health states from published literature. We used multi-way sensitivity analyses to examine impact of uncertainty in input parameters on cost-effectiveness of FLS. The model estimates that an FLS would result in 153 fewer fractures (109 hip, 5 wrist, 21 spine, 17 other), 37.43 more quality-adjusted life years (QALYs), and save $66,879 compared with typical postfracture care per every 10,000 postfracture patients. Doubling the cost of the FLS resulted in an incremental cost-effectiveness ratio (ICER) of $22,993 per QALY. The sensitivity analyses showed that results were robust to plausible ranges of input parameters; assuming the least favorable values of each of the major input parameters results in an ICER of $112,877 per QALY. An FLS targeting patients post-hip fracture should result in cost savings and reduced fractures under most scenarios.
Keywords: COST-EFFECTIVENESS; FRACTURE LIAISON SERVICE; HIP FRACTURE; OSTEOPOROSIS.
© 2014 American Society for Bone and Mineral Research.
Figures
Similar articles
-
Economic evaluation of a population-based osteoporosis intervention for outpatients with non-traumatic non-hip fractures: the "Catch a Break" 1i [type C] FLS.Osteoporos Int. 2017 Jun;28(6):1965-1977. doi: 10.1007/s00198-017-3986-3. Epub 2017 Mar 9. Osteoporos Int. 2017. PMID: 28275838 Free PMC article.
-
A 3i hip fracture liaison service with nurse and physician co-management is cost-effective when implemented as a standard clinical program.Arch Osteoporos. 2020 Jul 22;15(1):113. doi: 10.1007/s11657-020-00781-w. Arch Osteoporos. 2020. PMID: 32699946
-
Cost-effectiveness analysis of fracture liaison services: a Markov model using Dutch real-world data.Osteoporos Int. 2024 Feb;35(2):293-307. doi: 10.1007/s00198-023-06924-2. Epub 2023 Oct 3. Osteoporos Int. 2024. PMID: 37783759 Free PMC article.
-
Economic impact and cost-effectiveness of fracture liaison services: a systematic review of the literature.Osteoporos Int. 2018 Jun;29(6):1227-1242. doi: 10.1007/s00198-018-4411-2. Epub 2018 Feb 19. Osteoporos Int. 2018. PMID: 29460102
-
Fracture Liaison Services.Curr Opin Rheumatol. 2017 Jul;29(4):416-421. doi: 10.1097/BOR.0000000000000401. Curr Opin Rheumatol. 2017. PMID: 28426444 Review.
Cited by
-
Post-fracture pharmacotherapy for women with osteoporotic fracture: analysis of a managed care population in the USA.Osteoporos Int. 2014 Dec;25(12):2777-86. doi: 10.1007/s00198-014-2827-x. Epub 2014 Aug 12. Osteoporos Int. 2014. PMID: 25112720 Free PMC article.
-
Overdiagnosis of osteoporosis: fact or fallacy?Osteoporos Int. 2015 Aug;26(8):2051-4. doi: 10.1007/s00198-015-3220-0. Epub 2015 Jul 2. Osteoporos Int. 2015. PMID: 26134683 No abstract available.
-
The Potential Economic Benefits of an Alarm Service in Order Communication Systems in Korea: a Cost-Effectiveness Analysis of Less-Intensive Fracture Liaison Services Based on a Prospective Cohort Study.Calcif Tissue Int. 2022 Oct;111(4):380-390. doi: 10.1007/s00223-022-01000-z. Epub 2022 Jul 5. Calcif Tissue Int. 2022. PMID: 35790553
-
Validation of the SF-6D Health State Utilities Measure in Lower Extremity Sarcoma.Sarcoma. 2014;2014:450902. doi: 10.1155/2014/450902. Epub 2014 Mar 19. Sarcoma. 2014. PMID: 24771999 Free PMC article.
-
Fibrinolysis as a target to enhance osteoporotic fracture healing by vibration therapy in a metaphyseal fracture model.Bone Joint Res. 2021 Jan;10(1):41-50. doi: 10.1302/2046-3758.101.BJR-2020-0185.R1. Bone Joint Res. 2021. PMID: 33448865 Free PMC article.
References
-
- Board of Trustees FHITF Annual report. Services HaH. 2012:60. <zaq;2>.
-
- National Committee for Quality Assurance . 2010 The state of health care quality. NCQA; Washington, DC: 2010. p. 94.
-
- Recker RR, Lewiecki EM, Miller PD, Reiffel J. Safety of bisphosphonates in the treatment of osteoporosis. Am J Med. 2009;122(2 Suppl):S22–32. - PubMed
-
- Wells GA, Cranney A, Peterson J, et al. Alendronate for the primary and secondary prevention of osteoporotic fractures in postmenopausal women. Cochrane Database Syst Rev. 2008;(1):CD001155. - PubMed
-
- Dell R. Fracture prevention in Kaiser Permanente Southern California. Osteoporos Int. 2011;22(Suppl 3):457–60. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
