

Clinical outcomes among persons with pulmonary tuberculosis caused by Mycobacterium tuberculosis isolates with phenotypic heterogeneity in results of drug-susceptibility tests
- PMID: 24443546
- PMCID: PMC4017367
- DOI: 10.1093/infdis/jiu040
Clinical outcomes among persons with pulmonary tuberculosis caused by Mycobacterium tuberculosis isolates with phenotypic heterogeneity in results of drug-susceptibility tests
Abstract
Background: Patients with multidrug-resistant (MDR) tuberculosis may have phenotypic heterogeneity in results of drug-susceptibility tests (DSTs). However, the impact of this on clinical outcomes among patients treated for MDR tuberculosis is unknown.
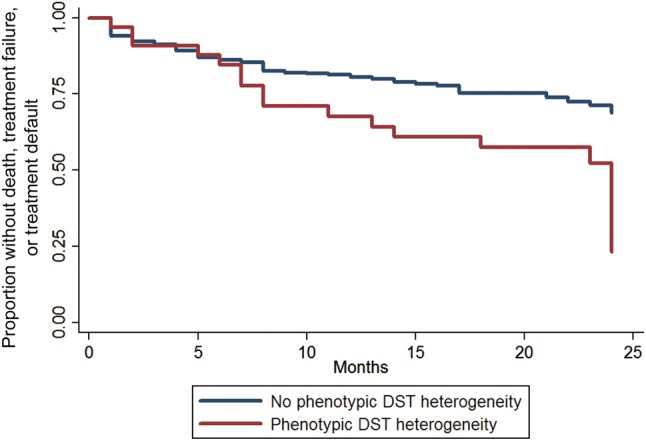
Methods: Phenotypic DST heterogeneity was defined as presence of at least 1 Mycobacterium tuberculosis isolate susceptible to rifampicin and isoniazid recovered <3 months after MDR tuberculosis treatment initiation from a patient with previous documented tuberculosis due to M. tuberculosis resistant to at least rifampicin and isoniazid. The primary outcome was defined as good (ie, cure or treatment completion) or poor (ie, treatment failure, treatment default, or death). A secondary outcome was time to culture conversion. Cox proportional hazard models were used to determine the association between phenotypic DST heterogeneity and outcomes.
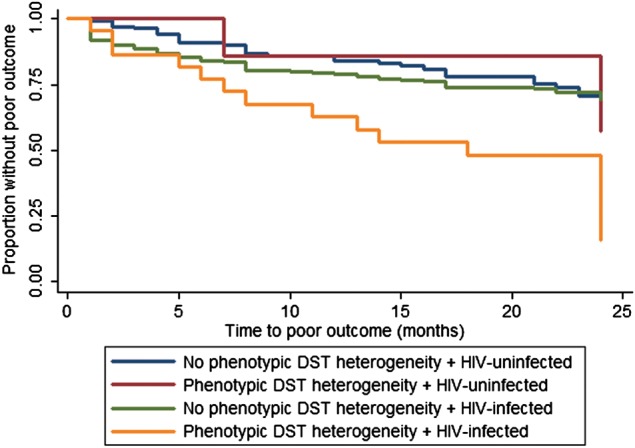
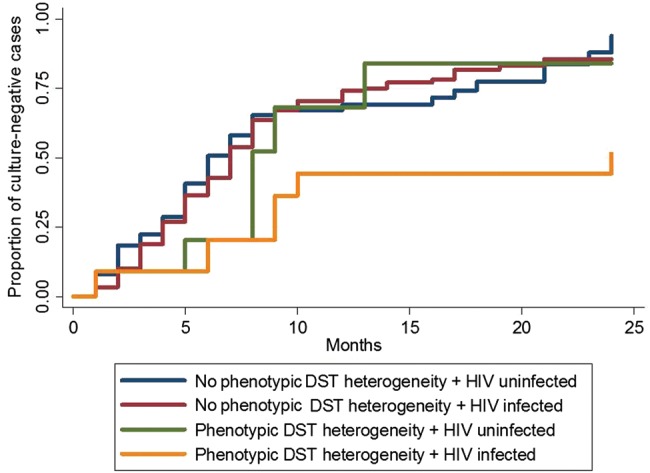
Results: Phenotypic DST heterogeneity was identified in 33 of 475 patients (7%) with MDR tuberculosis. Poor outcome occurred in 126 patients (28%). Overall, patients with MDR tuberculosis who had phenotypic DST heterogeneity were at greater risk of poor outcome than those with MDR tuberculosis but no phenotypic DST heterogeneity (adjusted hazard ratio [aHR], 2.1; 95% confidence interval [CI], 1.2-3.6). Among HIV-infected patients with MDR tuberculosis, the adjusted hazard for a poor outcome for those with phenotypic DST heterogeneity was 2.4 (95% CI, 1.3-4.2) times that for those without phenotypic DST heterogeneity, whereas among HIV-negative patients with MDR tuberculosis, the adjusted hazard for those with phenotypic DST heterogeneity was 1.5 (95% CI, .5-4.3) times that for those without phenotypic DST heterogeneity. HIV-infected patients with MDR tuberculosis with phenotypic DST heterogeneity also had a longer time to culture conversion than with HIV-infected patients with MDR tuberculosis without phenotypic DST heterogeneity (aHR, 2.9; 95% CI, 1.4-6.0).
Conclusions: Phenotypic DST heterogeneity among persons with HIV infection who are being treated for MDR tuberculosis is associated with poor outcomes and longer times to culture conversion.
Keywords: Tuberculosis; drug susceptibility testing; mixed infection, heteroresistance; multidrug-resistant tuberculosis; treatment outcome.
Figures
Comment in
-
Resistant plus susceptible tuberculosis: the undiscovered country.J Infect Dis. 2014 Jun 1;209(11):1682-4. doi: 10.1093/infdis/jiu078. Epub 2014 Feb 12. J Infect Dis. 2014. PMID: 24523512 No abstract available.
References
-
- Garcia de Viedma D, Marin M, Ruiz Serrano MJ, Alcala L, Bouza E. Polyclonal and compartmentalized infection by Mycobacterium tuberculosis in patients with both respiratory and extrarespiratory involvement. J Infect Dis. 2003;187:695–9. - PubMed
-
- Glynn JR, Yates MD, Crampin AC, et al. DNA fingerprint changes in tuberculosis: reinfection, evolution, or laboratory error? J Infect Dis. 2004;190:1158–66. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
