

Neurocognitive development in 22q11.2 deletion syndrome: comparison with youth having developmental delay and medical comorbidities
- PMID: 24445907
- PMCID: PMC4450860
- DOI: 10.1038/mp.2013.189
Neurocognitive development in 22q11.2 deletion syndrome: comparison with youth having developmental delay and medical comorbidities
Abstract
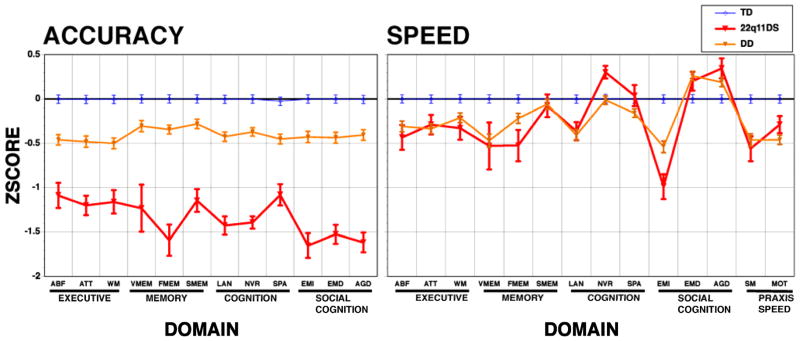
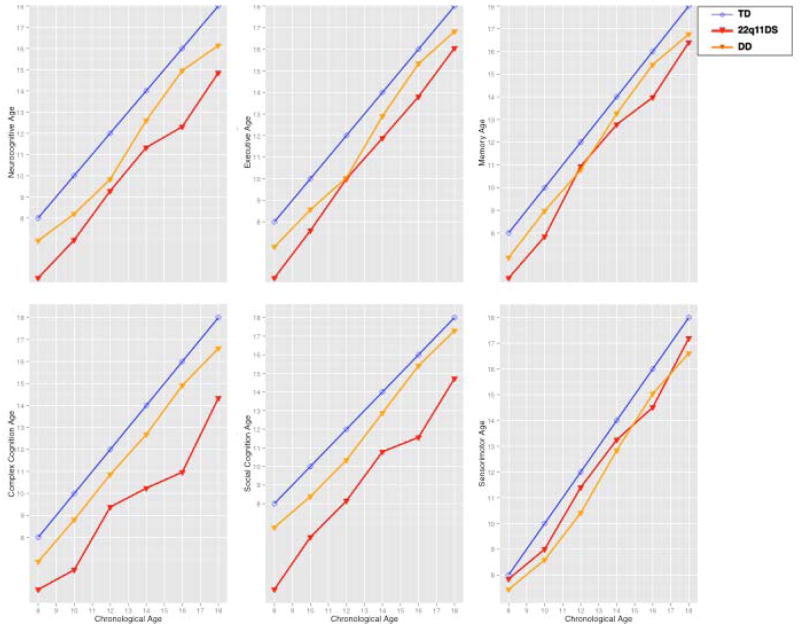
The 22q11.2 deletion syndrome (22q11DS) presents with medical and neuropsychiatric manifestations including neurocognitive deficits. Quantitative neurobehavioral measures linked to brain circuitry can help elucidate genetic mechanisms contributing to deficits. To establish the neurocognitive profile and neurocognitive 'growth charts', we compared cross-sectionally 137 individuals with 22q11DS ages 8-21 to 439 demographically matched non-deleted individuals with developmental delay (DD) and medical comorbidities and 443 typically developing (TD) participants. We administered a computerized neurocognitive battery that measures performance accuracy and speed in executive, episodic memory, complex cognition, social cognition and sensorimotor domains. The accuracy performance profile of 22q11DS showed greater impairment than DD, who were impaired relative to TD. Deficits in 22q11DS were most pronounced for face memory and social cognition, followed by complex cognition. Performance speed was similar for 22q11DS and DD, but 22q11DS individuals were differentially slower in face memory and emotion identification. The growth chart, comparing neurocognitive age based on performance relative to chronological age, indicated that 22q11DS participants lagged behind both groups from the earliest age assessed. The lag ranged from less than 1 year to over 3 years depending on chronological age and neurocognitive domain. The greatest developmental lag across the age range was for social cognition and complex cognition, with the smallest for episodic memory and sensorimotor speed, where lags were similar to DD. The results suggest that 22q11.2 microdeletion confers specific vulnerability that may underlie brain circuitry associated with deficits in several neuropsychiatric disorders, and therefore help identify potential targets and developmental epochs optimal for intervention.
Conflict of interest statement
The authors report no conflict of interest.
Figures
Similar articles
-
Neurocognitive profile in psychotic versus nonpsychotic individuals with 22q11.2 deletion syndrome.Eur Neuropsychopharmacol. 2016 Oct;26(10):1610-8. doi: 10.1016/j.euroneuro.2016.08.003. Epub 2016 Aug 12. Eur Neuropsychopharmacol. 2016. PMID: 27524298
-
Performance on a computerized neurocognitive battery in 22q11.2 deletion syndrome: A comparison between US and Israeli cohorts.Brain Cogn. 2016 Jul;106:33-41. doi: 10.1016/j.bandc.2016.02.002. Epub 2016 May 17. Brain Cogn. 2016. PMID: 27200494 Free PMC article.
-
The interaction between neurocognitive functioning, subthreshold psychotic symptoms and pharmacotherapy in 22q11.2 deletion syndrome: A longitudinal comparative study.Eur Psychiatry. 2018 Feb;48:20-26. doi: 10.1016/j.eurpsy.2017.10.010. Epub 2018 Jan 10. Eur Psychiatry. 2018. PMID: 29331595
-
Social cognitive impairment in 22q11 deletion syndrome: A review.Psychiatry Res. 2017 Jul;253:99-106. doi: 10.1016/j.psychres.2017.01.103. Epub 2017 Feb 23. Psychiatry Res. 2017. PMID: 28364592 Review.
-
[Neurocognitive and psychiatric management of the 22q11.2 deletion syndrome].Encephale. 2015 Jun;41(3):266-73. doi: 10.1016/j.encep.2014.10.005. Epub 2014 Dec 16. Encephale. 2015. PMID: 25523123 Review. French.
Cited by
-
An implicit and reliable neural measure quantifying impaired visual coding of facial expression: evidence from the 22q11.2 deletion syndrome.Transl Psychiatry. 2019 Feb 4;9(1):67. doi: 10.1038/s41398-019-0411-z. Transl Psychiatry. 2019. PMID: 30718458 Free PMC article.
-
Neuroanatomical Correlates of Cognitive Dysfunction in 22q11.2 Deletion Syndrome.Genes (Basel). 2024 Mar 30;15(4):440. doi: 10.3390/genes15040440. Genes (Basel). 2024. PMID: 38674375 Free PMC article. Review.
-
Childhood cognitive development in 22q11.2 deletion syndrome: case-control study.Br J Psychiatry. 2017 Oct;211(4):223-230. doi: 10.1192/bjp.bp.116.195651. Epub 2017 Sep 7. Br J Psychiatry. 2017. PMID: 28882829 Free PMC article.
-
Genes To Mental Health (G2MH): A Framework to Map the Combined Effects of Rare and Common Variants on Dimensions of Cognition and Psychopathology.Am J Psychiatry. 2022 Mar;179(3):189-203. doi: 10.1176/appi.ajp.2021.21040432. Am J Psychiatry. 2022. PMID: 35236119 Free PMC article. Review.
-
Early language measures associated with later psychosis features in 22q11.2 deletion syndrome.Am J Med Genet B Neuropsychiatr Genet. 2020 Sep;183(6):392-400. doi: 10.1002/ajmg.b.32812. Epub 2020 Jul 27. Am J Med Genet B Neuropsychiatr Genet. 2020. PMID: 32715620 Free PMC article.
References
-
- Antshel KM, Fremont W, Roizen NJ, Shprintzen R, Higgins AM, Dhamoon A, et al. ADHD, major depressive disorder, and simple phobias are prevalent psychiatric conditions in youth with velo cardio facial syndrome. J Am Acad Child Adolesc Psychiatry. 2006;45:596–603. - PubMed
-
- Fabbro A, Rizzi E, Schneider M, Debbane M, Eliez S. Depression and anxiety disorders in children and adolescents with velo-cardio-facial syndrome (VCFS) Eur Child Adolesc Psychiatry. 2012;21:379–385. - PubMed
-
- Gothelf D, Feinstein C, Thompson T, Gu E, Penniman L, Van Stone E, et al. Risk factors for the emergence of psychotic disorders in adolescents with 22q11. 2 deletion syndrome. Am J Psychiatry. 2007;164:663–669. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
