

Variation in performance of candidate surgical quality measures for muscle-invasive bladder cancer by hospital type
- PMID: 24447637
- PMCID: PMC4472465
- DOI: 10.1111/bju.12638
Variation in performance of candidate surgical quality measures for muscle-invasive bladder cancer by hospital type
Abstract
Objective: To test the association between hospital type and performance of candidate quality measures for treatment of muscle-invasive bladder cancer (MIBC) using a large national tumour registry. Proposed quality measures include receipt of neoadjuvant chemotherapy, timely treatment, adequate lymph node dissection, and continent urinary diversion.
Patients and methods: Using the National Cancer Database, patients with stage ≥II urothelial carcinoma treated with radical cystectomy (RC) from 2003 to 2010 were identified. Hospitals were grouped by type and annual RC volume: community, comprehensive low volume (CLV), comprehensive high volume (CHV), academic low volume (ALV), and academic high volume (AHV) groups. Logistic regression models were used to test the association between hospital group and performance of quality measures, adjusting for year, demographic, and clinical/pathological characteristics; generalised estimating equations were fitted to the models to adjust for clustering at the hospital level.
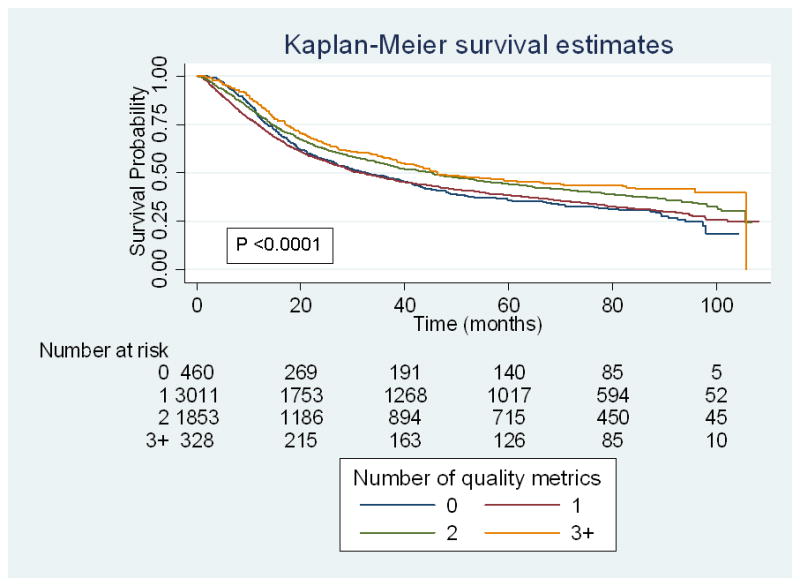
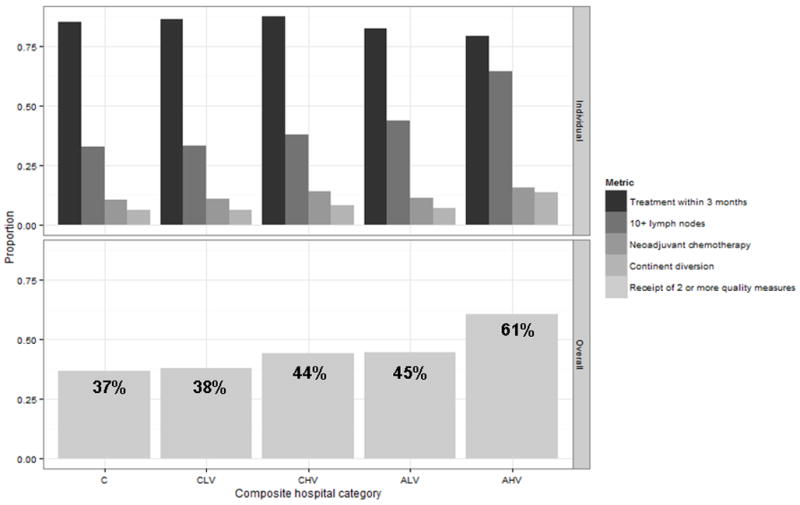
Results: In all, 23 279 patients underwent RC at community (12.4%), comprehensive (CLV 38%, CHV 5%), and academic (ALV 17%, AHV 28%) hospitals. While only 0.8% (175) of patients met all four quality criteria, 61% of patients treated at AHV hospitals met two or more quality metric indicators compared with ALV (45%), CHV (44%), CLV (38%), and community (37%) hospitals (P < 0.001). After adjustment, patients were more likely to receive two or more quality measures when treated at AHV (odds ratio [OR] 2.4, confidence interval [CI] 2.0-2.9), ALV (OR 1.3, CI 1.1-1.6), and CHV (OR 1.3, CI 1.03-1.7) hospitals compared with community hospitals.
Conclusions: Patients undergoing RC at AHV hospitals were more likely to meet quality criteria. However, performance remains low across hospital types, highlighting the opportunity to improve quality of care for MIBC.
Keywords: bladder cancer; hospital type; quality measures; radical cystectomy; surgical volume.
© 2014 The Authors. BJU International © 2014 BJU International.
Conflict of interest statement
No financial disclosures or conflicts of interest.
Figures
Comment in
-
Re: Variation in Performance of Candidate Surgical Quality Measures for Muscle-Invasive Bladder Cancer by Hospital Type.J Urol. 2016 Jun;195(6):1721-2. doi: 10.1016/j.juro.2016.03.025. Epub 2016 Mar 19. J Urol. 2016. PMID: 27191066 No abstract available.
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA: a cancer journal for clinicians. 2013 Jan;63:11–30. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
