

Treatment of postmastectomy pain with ambulatory continuous paravertebral nerve blocks: a randomized, triple-masked, placebo-controlled study
- PMID: 24448512
- PMCID: PMC3944096
- DOI: 10.1097/AAP.0000000000000035
Treatment of postmastectomy pain with ambulatory continuous paravertebral nerve blocks: a randomized, triple-masked, placebo-controlled study
Abstract
Background: We aimed to determine with this randomized, triple-masked, placebo-controlled study if benefits are afforded by adding a multiple-day, ambulatory, continuous ropivacaine paravertebral nerve block to a single-injection ropivacaine paravertebral block after mastectomy.
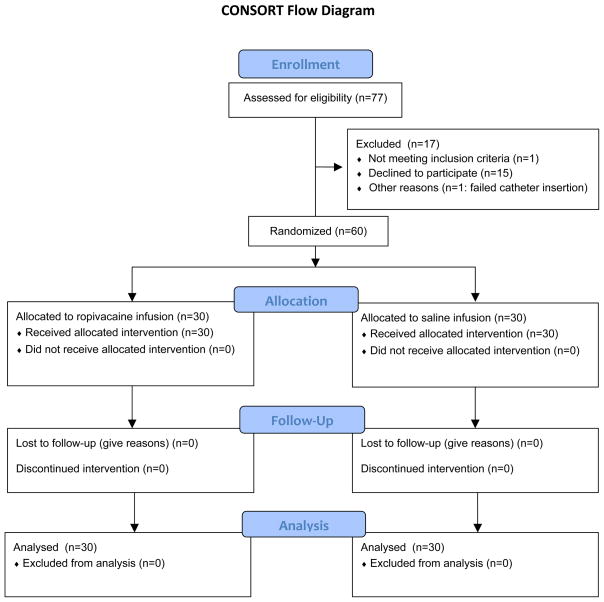
Methods: Preoperatively, 60 subjects undergoing unilateral (n = 24) or bilateral (n = 36) mastectomy received either unilateral or bilateral paravertebral perineural catheter(s), respectively, inserted between the third and fourth thoracic transverse process(es). All subjects received an initial bolus of ropivacaine 0.5% (15 mL) via the catheter(s). Subjects were randomized to receive either perineural ropivacaine 0.4% or normal saline using portable infusion pump(s) [5 mL/h basal; 300 mL reservoir(s)]. Subjects remained hospitalized for at least 1 night and were subsequently discharged home where the catheter(s) were removed on postoperative day (POD) 3. Subjects were contacted by telephone on PODs 1, 4, 8, and 28. The primary end point was average pain (scale, 0-10) queried on POD 1.
Results: Average pain queried on POD 1 for subjects receiving perineural ropivacaine (n = 30) was a median (interquartile) of 2 (0-3), compared with 4 (1-5) for subjects receiving saline (n = 30; 95% confidence interval difference in medians, -4.0 to -0.3; P = 0.021]. During this same period, subjects receiving ropivacaine experienced a lower severity of breakthrough pain (5 [3-6] vs 7 [5-8]; P = 0.046) as well. As a result, subjects receiving perineural ropivacaine experienced less pain-induced physical and emotional dysfunction, as measured with the Brief Pain Inventory (lower score = less dysfunction): 14 (4-37) versus 57 (8-67) for subjects receiving perineural saline (P = 0.012). For the subscale that measures the degree of interference of pain on 7 domains, such as general activity and relationships, subjects receiving perineural saline reported a median score 10 times higher (more dysfunction) than those receiving ropivacaine (3 [0-24] vs 33 [0-44]; P = 0.035). In contrast, after infusion discontinuation, there were no statistically significant differences detected between treatment groups.
Conclusions: After mastectomy, adding a multiple-day, ambulatory, continuous ropivacaine infusion to a single-injection ropivacaine paravertebral nerve block results in improved analgesia and less functional deficit during the infusion. However, no benefits were identified after infusion discontinuation.
Conflict of interest statement
The authors declare no conflict of interest.
Comment in
-
Primum non nocere.Reg Anesth Pain Med. 2014 Mar-Apr;39(2):87-8. doi: 10.1097/AAP.0000000000000060. Reg Anesth Pain Med. 2014. PMID: 24553303 No abstract available.
References
-
- Howlader N, Noone AM, Krapcho M, et al., editors. SEER Cancer Statistics Review, 1975–2009. Bethesda, MD: 2012.
-
- Habermann EB, Abbott A, Parsons HM, Virnig BA, Al-Refaie WB, Tuttle TM. Are mastectomy rates really increasing in the United States? J Clin Oncol. 2010;28:3437–3441. - PubMed
-
- Cepeda MS, Africano JM, Polo R, Alcala R, Carr DB. What decline in pain intensity is meaningful to patients with acute pain? Pain. 2003;105:151–157. - PubMed
-
- Kairaluoma PM, Bachmann MS, Korpinen AK, Rosenberg PH, Pere PJ. Single-injection paravertebral block before general anesthesia enhances analgesia after breast cancer surgery with and without associated lymph node biopsy. Anesth Analg. 2004;99:1837–1843. - PubMed
-
- Klein SM, Bergh A, Steele SM, Georgiade GS, Greengrass RA. Thoracic paravertebral block for breast surgery. Anesth Analg. 2000;90:1402–1405. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials