

Effects of topiroxostat on the serum urate levels and urinary albumin excretion in hyperuricemic stage 3 chronic kidney disease patients with or without gout
- PMID: 24448692
- PMCID: PMC4271138
- DOI: 10.1007/s10157-014-0935-8
Effects of topiroxostat on the serum urate levels and urinary albumin excretion in hyperuricemic stage 3 chronic kidney disease patients with or without gout
Abstract
Background: Topiroxostat, a selective xanthine oxidase inhibitor, shows effective reduction in the serum urate level in hyperuricemic patients with or without gout. The objective of this study was to evaluate the efficacy and safety of topiroxostat in hyperuricemic stage 3 chronic kidney disease patients with or without gout.
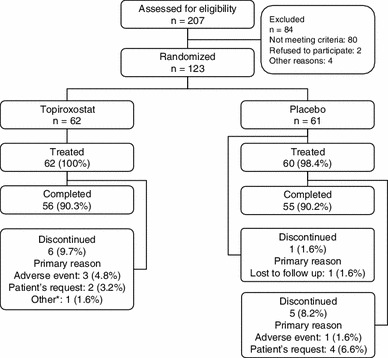
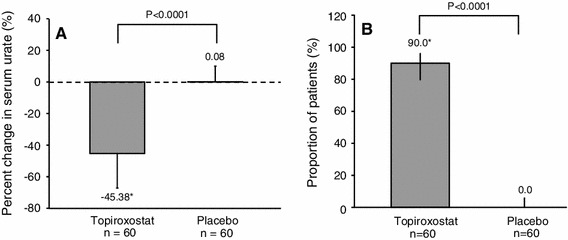
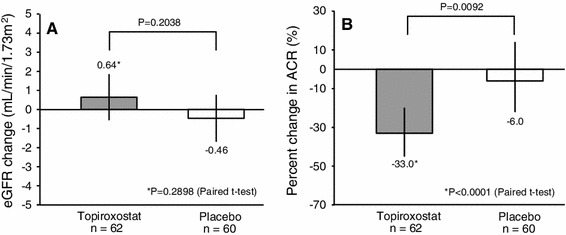
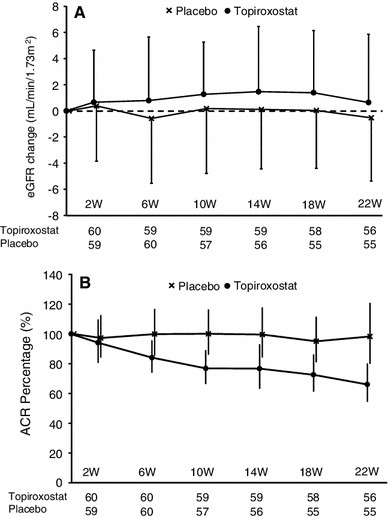
Methods: The study design was a 22-week, randomized, multicenter, double-blind study. The enrolled patients were randomly assigned to treatment with topiroxostat 160 mg/day (n = 62) or to the placebo (n = 61). The endpoints were the percent change in the serum urate level, change in the estimated glomerular filtration rate, the urinary albumin-to-creatinine ratio, the proportion of patients with serum urate levels of 356.88 μmol/L or less, blood pressure, and serum adiponectin.
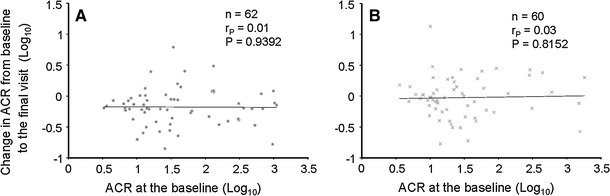
Results: After 22 weeks, although the changes in the estimated glomerular filtration rate and blood pressure were not significant, the percent change in the serum urate level (-45.38 vs. -0.08 %, P < 0.0001) and the percent change in urinary albumin-to-creatinine ratio (-33.0 vs. -6.0 %, P = 0.0092) were found to have decreased in the topiroxostat as compared with the placebo. Although the incidence of 'alanine aminotransferase increased' was higher in the topiroxostat, serious adverse event rates were similar in the two groups.
Conclusion: Topiroxostat 160 mg effectively reduced the serum urate level in the hyperuricemic stage 3 chronic kidney disease patients with or without gout.
Figures
References
-
- Chang HY, Tung CW, Lee PH, et al. Hyperuricemia as an independent risk factor of chronic kidney disease in middle-aged and elderly population. Am J Med Sci. 2010;339:509–515. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
