

Psychological treatments for depression and anxiety in dementia and mild cognitive impairment
- PMID: 24449085
- PMCID: PMC6465082
- DOI: 10.1002/14651858.CD009125.pub2
Psychological treatments for depression and anxiety in dementia and mild cognitive impairment
Update in
-
Psychological treatments for depression and anxiety in dementia and mild cognitive impairment.Cochrane Database Syst Rev. 2022 Apr 25;4(4):CD009125. doi: 10.1002/14651858.CD009125.pub3. Cochrane Database Syst Rev. 2022. PMID: 35466396 Free PMC article.
Abstract
Background: Experiencing anxiety and depression is very common in people with dementia and mild cognitive impairment (MCI). Psychological interventions have been suggested as a potential treatment for these populations. Current research suggests that people with dementia and MCI have limited opportunities for psychological treatments aimed at improving their well-being. A systematic review of the evidence on their effectiveness is likely to be useful in terms of improving outcomes for patients and for future recommendations for practice.
Objectives: The main objective of this review was to assess the effectiveness of psychological interventions in reducing anxiety and depression in people with dementia or mild cognitive impairment (MCI).
Search methods: We searched the Cochrane Dementia and Cognitive Improvement Group Specialized Register and additional sources for both published and unpublished data.
Selection criteria: We included randomised controlled trials (RCTs) comparing a psychological intervention with usual care or a placebo intervention (social contact control) in people with dementia or MCI.
Data collection and analysis: Two review authors worked independently to select trials, extract data and assess studies for risk of bias, using a data extraction form. We contacted authors when further information was not available from the published articles.
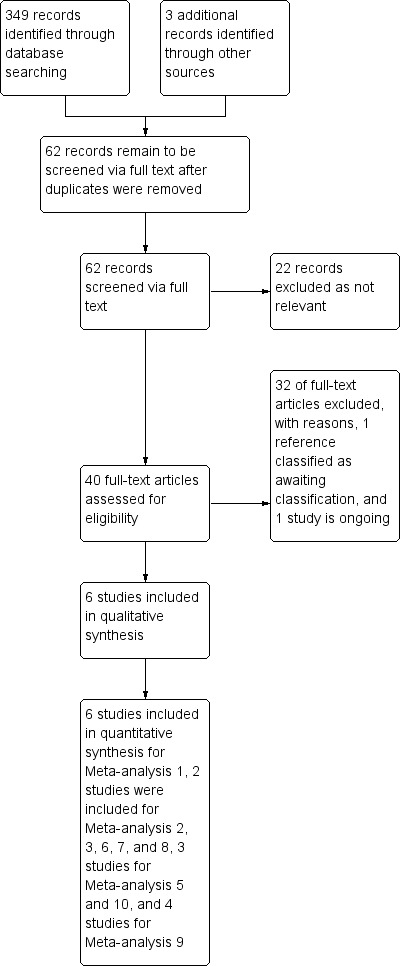
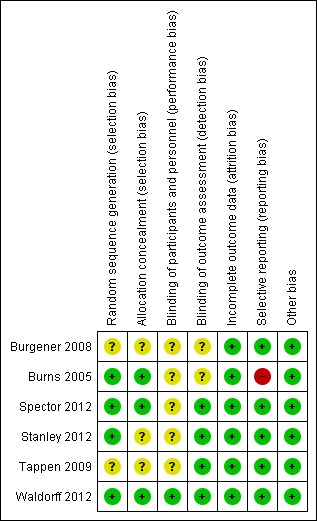
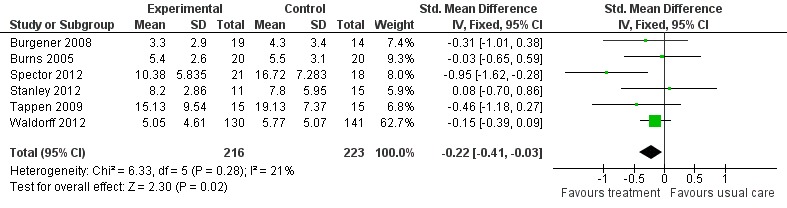
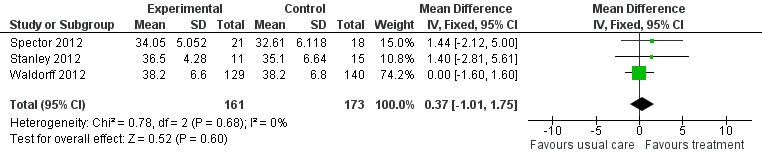
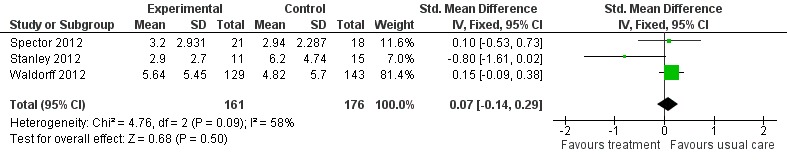
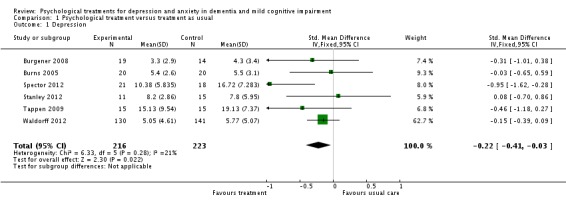
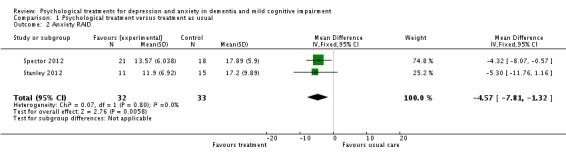
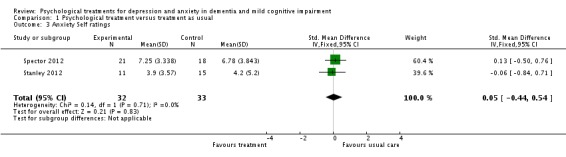
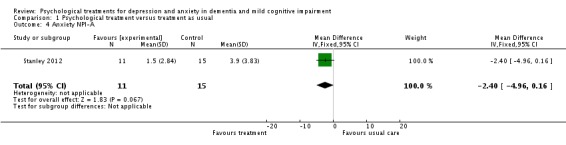
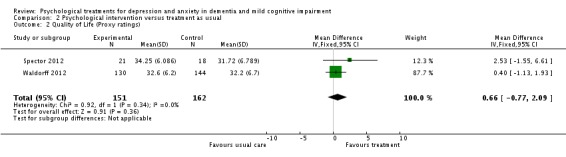
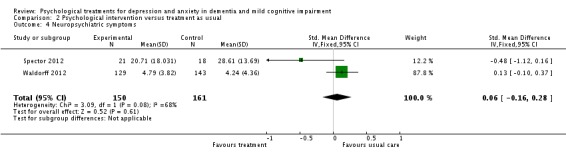
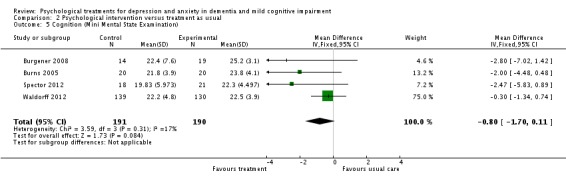
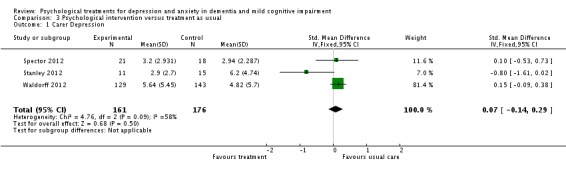
Main results: Six RCTs involving 439 participants with dementia were included in the review, but no studies of participants with MCI were identified. The studies included people with dementia living in the community or in nursing home care and were carried out in several countries. Only one of the studies was classified as low risk of bias. Five studies were at unclear or high risk of bias due to uncertainties around randomisation, blinding and selective reporting of results. The studies used the different psychological approaches of cognitive behavioural therapy (CBT), interpersonal therapy and counselling. Two studies were of multimodal interventions including a specific psychological therapy. The comparison groups received either usual care, attention-control educational programs, diagnostic feedback or services slightly above usual care.Meta-analysis showed a positive effect of psychological treatments on depression (6 trials, 439 participants, standardised mean difference (SMD) -0.22; 95% confidence interval (CI) -0.41 to -0.03, moderate quality evidence) and on clinician-rated anxiety (2 trials, 65 participants, mean difference (MD) -4.57; 95% CI -7.81 to -1.32, low quality evidence), but not on self-rated anxiety (2 trials, SMD 0.05; 95% CI -0.44 to 0.54) or carer-rated anxiety (1 trial, MD -2.40; 95% CI -4.96 to 0.16). Results were compatible with both benefit and harm on the secondary outcomes of patient quality of life, activities of daily living (ADLs), neuropsychiatric symptoms and cognition, or on carers' self-rated depressive symptoms, but most of the studies did not measure these outcomes. There were no reports of adverse events.
Authors' conclusions: We found evidence that psychological interventions added to usual care can reduce symptoms of depression and clinician-rated anxiety for people with dementia. We conclude that psychological interventions have the potential to improve patient well-being. Further high quality studies are needed to investigate which treatments are most effective and to evaluate the effect of psychological interventions in people with MCI.
Conflict of interest statement
The second, third and fourth author of this review are investigators in one of the included studies. There are no other known conflicts of interest.
Figures










Comment in
-
Treating depression and anxiety in people with dementia.Nurs Times. 2016 Apr 20-26;112(16):20. Nurs Times. 2016. PMID: 27295801 No abstract available.
Similar articles
-
Psychological treatments for depression and anxiety in dementia and mild cognitive impairment.Cochrane Database Syst Rev. 2022 Apr 25;4(4):CD009125. doi: 10.1002/14651858.CD009125.pub3. Cochrane Database Syst Rev. 2022. PMID: 35466396 Free PMC article.
-
Music-based therapeutic interventions for people with dementia.Cochrane Database Syst Rev. 2025 Mar 7;3(3):CD003477. doi: 10.1002/14651858.CD003477.pub5. Cochrane Database Syst Rev. 2025. PMID: 40049590
-
Non-pharmacological interventions for somatoform disorders and medically unexplained physical symptoms (MUPS) in adults.Cochrane Database Syst Rev. 2014 Nov 1;2014(11):CD011142. doi: 10.1002/14651858.CD011142.pub2. Cochrane Database Syst Rev. 2014. PMID: 25362239 Free PMC article.
-
E-Health interventions for anxiety and depression in children and adolescents with long-term physical conditions.Cochrane Database Syst Rev. 2018 Aug 15;8(8):CD012489. doi: 10.1002/14651858.CD012489.pub2. Cochrane Database Syst Rev. 2018. PMID: 30110718 Free PMC article.
-
Educational interventions for the management of cancer-related fatigue in adults.Cochrane Database Syst Rev. 2016 Nov 24;11(11):CD008144. doi: 10.1002/14651858.CD008144.pub2. Cochrane Database Syst Rev. 2016. PMID: 27883365 Free PMC article.
Cited by
-
Computerized assessment of communication for cognitive stimulation for people with cognitive decline using spectral-distortion measures and phylogenetic inference.PLoS One. 2015 Mar 24;10(3):e0118739. doi: 10.1371/journal.pone.0118739. eCollection 2015. PLoS One. 2015. PMID: 25803586 Free PMC article.
-
Developing an ontology of non-pharmacological treatment for emotional and mood disturbances in dementia.Sci Rep. 2024 Jan 22;14(1):1937. doi: 10.1038/s41598-023-46226-5. Sci Rep. 2024. PMID: 38253678 Free PMC article.
-
Effects of Tianeptine Treatment on Depression and Cognitive Function in Patients with Alzheimer's Disease: A 12-Month Retrospective Observational Study.J Alzheimers Dis. 2022;88(2):707-720. doi: 10.3233/JAD-215630. J Alzheimers Dis. 2022. PMID: 35694919 Free PMC article.
-
The Effect of Cognitive Intervention on Cognitive Improvement in Patients with Dementia.Dement Neurocogn Disord. 2018 Mar;17(1):23-31. doi: 10.12779/dnd.2018.17.1.23. Epub 2018 Mar 14. Dement Neurocogn Disord. 2018. PMID: 30906388 Free PMC article.
-
Effectiveness of Early Multimodal Non-pharmacological Interventions in Cognitive Preservation in the Elderly.Am J Alzheimers Dis Other Demen. 2024 Jan-Dec;39:15333175241256803. doi: 10.1177/15333175241256803. Am J Alzheimers Dis Other Demen. 2024. PMID: 38798013 Free PMC article.
References
References to studies included in this review
-
- Burns A, Guthrie E, Marino‐Francis F, Busby C, Morris J, Russell E, et al. Brief psychotherapy in Alzheimer's disease: randomised controlled trial. The British Journal of Psychiatry 2005;187:143‐7. - PubMed
-
- Tappen RM, Williams CL. Therapeutic conversation to improve mood in nursing home residents with Alzheimer’s disease. Research in Gerontological Nursing 2009;2:267‐75. - PubMed
References to studies excluded from this review
-
- Abraham IL, Neundorfer MM, Currie LJ. Effects of group interventions on cognition and depression in nursing home residents. Nursing Research 1992;41:196‐202. - PubMed
-
- Beck, C, Vogelpohl, T, Rasin, J, Topps, J, O’Sullivan, P, Walls, R, et al. Effects of behavioral interventions on disruptive behavior and affect in demented nursing home residents. Nursing Research 2002;51(4):219‐28. - PubMed
-
- Brodaty H, Draper BM, Millar J, Low L, Lie D, Sharah S, et al. Randomized controlled trial of different models of care for nursing home residents with dementia complicated by depression or psychosis. Journal of Clinical Psychiatry 2003;64:63‐72. - PubMed
-
- Cheston R, Jones K, Gilliard J. Group psychotherapy and people with dementia. Aging and Mental Health2003; Vol. 7:452‐61. - PubMed
-
- Dartigues JF. Efficacy Assessment of Three Non Pharmacological Therapies in Alzheimer's Disease (ETNA3). Trials Register.
References to studies awaiting assessment
-
- Carreel C. Value of conversation groups in institutions for the elderly. Revue de Laryngologie 1990;111:319‐23. - PubMed
References to ongoing studies
-
- Forstmeier S. Cognitive‐behavioral treatment for mild Alzheimer's patients and their caregivers. Clinical Trials Register2011.
Additional references
-
- Absher JR, Cummings JL. Cognitive and noncognitive aspects of dementia syndromes: An overview. In: Burns A, Levy R editor(s). Dementia. London: Chapman & Hall Medical, 1994.
-
- Alexopoulos GS, Abrams RC, Young RC. Cornell Scale for Depression in Dementia. Biological Psychiatry 1988;23:271‐84. - PubMed
-
- Alexopoulos GS, Jeste DV, Chung H, Carpenter D, Ross R, Docherty JP. The expert consensus guideline series. Treatment of dementia and its behavioral disturbances. Introduction: methods, commentary, and summary. Postgraduate Medicine 2005;Spec No:6‐22. - PubMed
-
- Azermai M, Petrovic M, Elseviers MM, Bourgeois J, Bortel LM, Vander Stichele RH. Systematic appraisal of dementia guidelines for the management of behavioural and psychological symptoms. Ageing Research Reviews 2012;11:78‐86. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical