

Telehealth personalized cancer risk communication to motivate colonoscopy in relatives of patients with colorectal cancer: the family CARE Randomized controlled trial
- PMID: 24449229
- PMCID: PMC3927734
- DOI: 10.1200/JCO.2013.51.6765
Telehealth personalized cancer risk communication to motivate colonoscopy in relatives of patients with colorectal cancer: the family CARE Randomized controlled trial
Abstract
Purpose: The rate of adherence to regular colonoscopy screening in individuals at increased familial risk of colorectal cancer (CRC) is suboptimal, especially among rural and other geographically underserved populations. Remote interventions may overcome geographic and system-level barriers. We compared the efficacy of a telehealth-based personalized risk assessment and communication intervention with a mailed educational brochure for improving colonoscopy screening among at-risk relatives of patients with CRC.
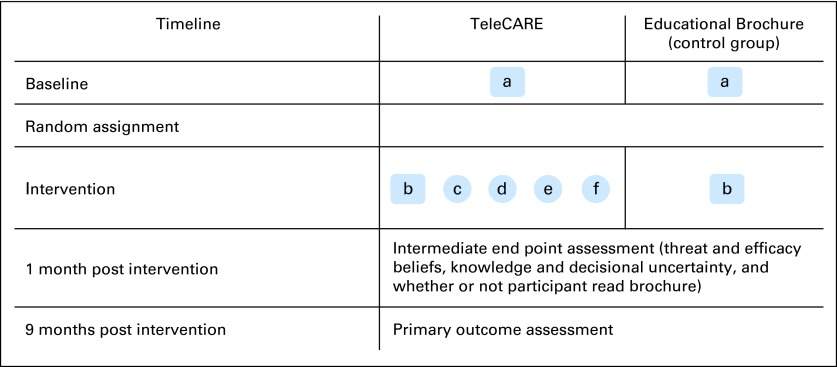
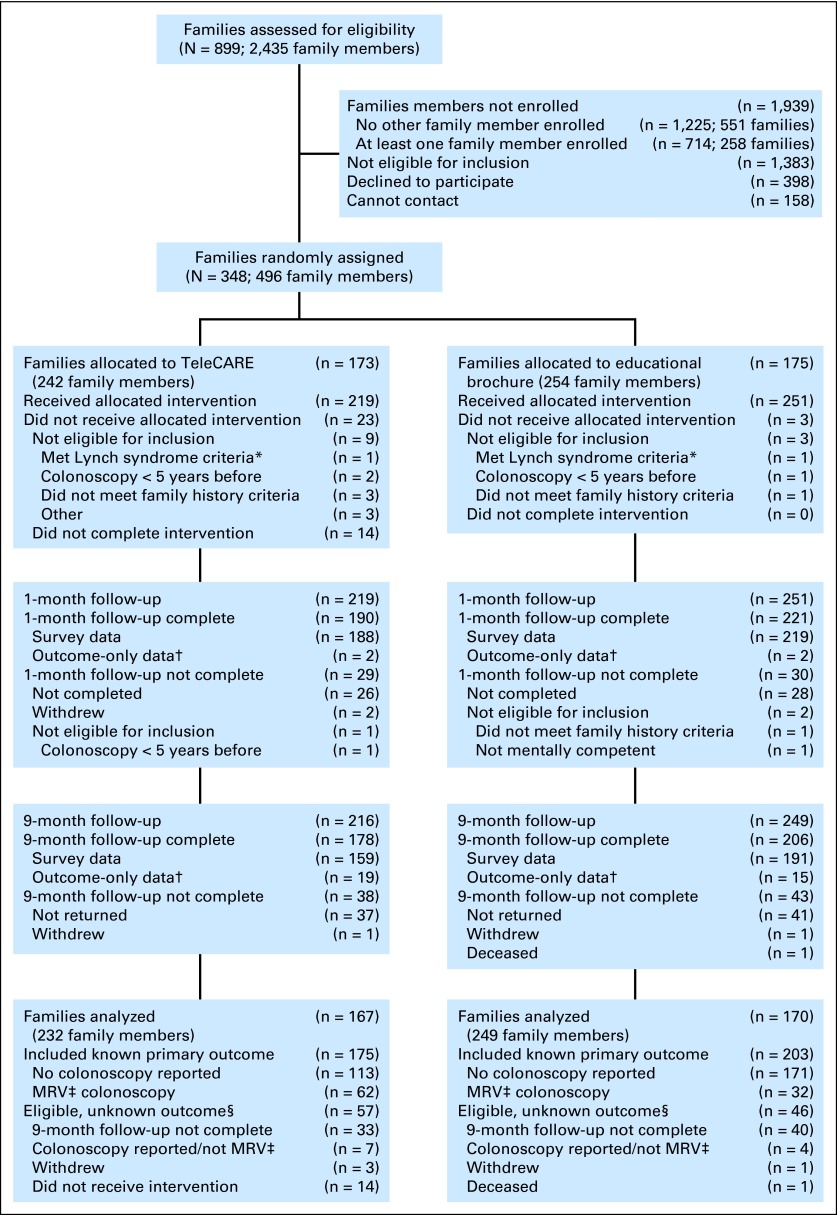
Methods: Eligible individuals age 30 to 74 years who were not up-to-date with risk-appropriate screening and were not candidates for genetic testing were recruited after contacting patients with CRC or their next of kin in five states. Enrollees were randomly assigned as family units to either an active, personalized intervention that incorporated evidence-based risk communication and behavior change techniques, or a mailed educational brochure. The primary outcome was medically verified colonoscopy within 9 months of the intervention.
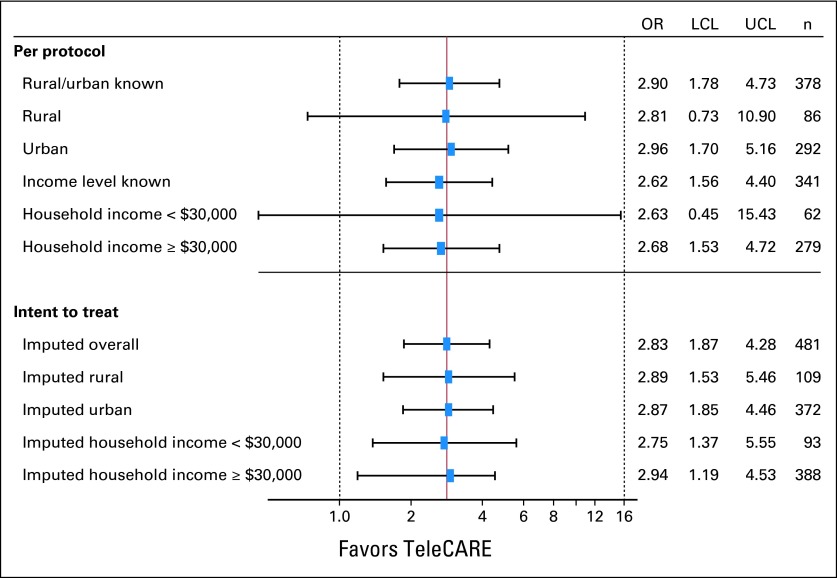
Results: Of the 481 eligible and randomly assigned at-risk relatives, 79.8% completed the outcome assessments within 9 months; 35.4% of those in the personalized intervention group and 15.7% of those in the comparison group obtained a colonoscopy. In an intent-to-treat analysis, the telehealth group was almost three times as likely to get screened as the low-intensity comparison group (odds ratio, 2.83; 95% CI, 1.87 to 4.28; P < .001). Persons residing in rural areas and those with lower incomes benefitted at the same level as did urban residents.
Conclusion: Remote personalized interventions that consider family history and incorporate evidence-based risk communication and behavior change strategies may promote risk-appropriate screening in close relatives of patients with CRC.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Similar articles
-
Efficacy of a Telehealth Intervention on Colonoscopy Uptake When Cost Is a Barrier: The Family CARE Cluster Randomized Controlled Trial.Cancer Epidemiol Biomarkers Prev. 2015 Sep;24(9):1311-8. doi: 10.1158/1055-9965.EPI-15-0150. Epub 2015 Jun 22. Cancer Epidemiol Biomarkers Prev. 2015. PMID: 26101306 Free PMC article. Clinical Trial.
-
Comparative effectiveness of fecal immunochemical test outreach, colonoscopy outreach, and usual care for boosting colorectal cancer screening among the underserved: a randomized clinical trial.JAMA Intern Med. 2013 Oct 14;173(18):1725-32. doi: 10.1001/jamainternmed.2013.9294. JAMA Intern Med. 2013. PMID: 23921906 Free PMC article. Clinical Trial.
-
Improving adherence to surveillance and screening recommendations for people with colorectal cancer and their first degree relatives: a randomized controlled trial.BMC Cancer. 2012 Feb 8;12:62. doi: 10.1186/1471-2407-12-62. BMC Cancer. 2012. PMID: 22314015 Free PMC article. Clinical Trial.
-
Effectiveness of tailored communication intervention in increasing colonoscopy screening rates amongst first-degree relatives of individuals with colorectal cancer: A systematic review and meta-analysis.Int J Nurs Stud. 2020 Jan;101:103397. doi: 10.1016/j.ijnurstu.2019.103397. Epub 2019 Aug 16. Int J Nurs Stud. 2020. PMID: 31683227
-
Effects of Family History on Relative and Absolute Risks for Colorectal Cancer: A Systematic Review and Meta-Analysis.Clin Gastroenterol Hepatol. 2019 Dec;17(13):2657-2667.e9. doi: 10.1016/j.cgh.2019.09.007. Epub 2019 Sep 13. Clin Gastroenterol Hepatol. 2019. PMID: 31525516
Cited by
-
The Impact of Information Technology on Patient Engagement and Health Behavior Change: A Systematic Review of the Literature.JMIR Med Inform. 2016 Jan 21;4(1):e1. doi: 10.2196/medinform.4514. JMIR Med Inform. 2016. PMID: 26795082 Free PMC article.
-
Interventions to Increase Colorectal Cancer Screening Uptake in Rural Settings: A Scoping Review.Prev Chronic Dis. 2025 Jul 17;22:E44. doi: 10.5888/pcd22.250025. Prev Chronic Dis. 2025. PMID: 40674655 Free PMC article.
-
Predictors of Response Outcomes for Research Recruitment Through a Central Cancer Registry: Evidence From 17 Recruitment Efforts for Population-Based Studies.Am J Epidemiol. 2019 May 1;188(5):928-939. doi: 10.1093/aje/kwz011. Am J Epidemiol. 2019. PMID: 30689685 Free PMC article.
-
Quality measures in the delivery of equitable endoscopic care to traditionally underserved patients in the United States.Gastrointest Endosc. 2025 Apr;101(4):733-744. doi: 10.1016/j.gie.2024.06.030. Epub 2024 Oct 18. Gastrointest Endosc. 2025. PMID: 39425707 Free PMC article. No abstract available.
-
Patient feedback and early outcome data with a novel tiered-binned model for multiplex breast cancer susceptibility testing.Genet Med. 2016 Jan;18(1):25-33. doi: 10.1038/gim.2015.19. Epub 2015 Apr 2. Genet Med. 2016. PMID: 25834950
References
-
- Lichtenstein P, Holm NV, Verkasalo PK, et al. Environmental and heritable factors in the causation of cancer: Analyses of cohorts of twins from Sweden, Denmark, and Finland. N Engl J Med. 2000;343:78–85. - PubMed
-
- Kerber RA, Neklason DW, Samowitz WS, et al. Frequency of familial colon cancer and hereditary nonpolyposis colorectal cancer (Lynch syndrome) in a large population database. Fam Cancer. 2005;4:239–244. - PubMed
-
- Butterworth AS, Higgins JP, Pharoah P. Relative and absolute risk of colorectal cancer for individuals with a family history: A meta-analysis. Eur J Cancer. 2006;42:216–227. - PubMed
-
- Johns LE, Houlston RS. A systematic review and meta-analysis of familial colorectal cancer risk. Am J Gastroenterol. 2001;96:2992–3003. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
