

Preterm birth by vacuum extraction and neonatal outcome: a population-based cohort study
- PMID: 24450413
- PMCID: PMC3900732
- DOI: 10.1186/1471-2393-14-42
Preterm birth by vacuum extraction and neonatal outcome: a population-based cohort study
Abstract
Background: Very few studies have investigated the neonatal outcomes after vacuum extraction delivery (VE) in the preterm period and the results of these studies are inconclusive. The objective of this study was to describe the use of VE for preterm delivery in Sweden and to compare rates of neonatal complications after preterm delivery by VE to those found after cesarean section during labor (CS) or unassisted vaginal delivery (VD).
Methods: Data was obtained from Swedish national registers. In a population-based cohort from 1999 to 2010, all live-born, singleton preterm infants in a non-breech presentation at birth, born after onset of labor (either spontaneously, by induction, or by rupture of membranes) by VD, CS, or VE were included, leaving a study population of 40,764 infants. Logistic regression analyses were used to calculate adjusted odds ratios (AOR), using unassisted vaginal delivery as reference group.
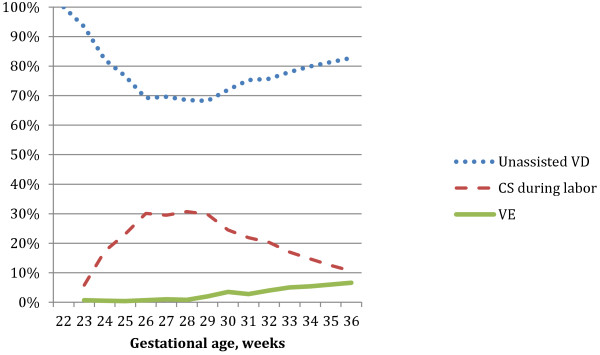
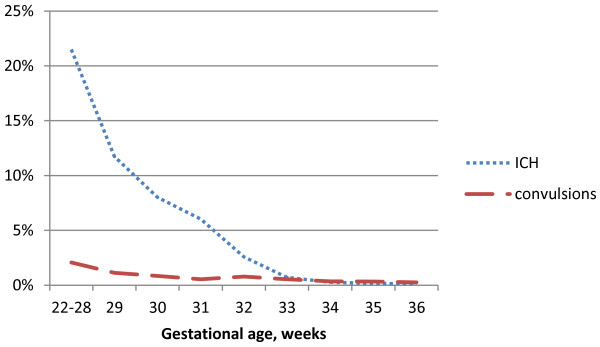
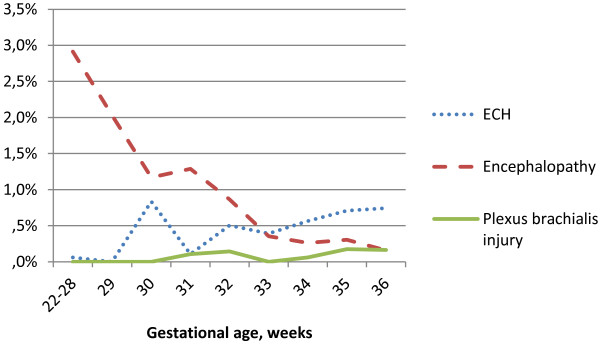
Results: VE was used in 5.7% of the preterm deliveries, with lower rates in earlier gestations. Overall, intracranial hemorrhage (ICH) occurred in 1.51%, extracranial hemorrhage (ECH) in 0.64%, and brachial plexus injury in 0.13% of infants. Infants delivered by VE had higher risks for ICH (AOR = 1.84 (95% CI: 1.09-3.12)), ECH (AOR = 4.48 (95% CI: 2.84-7.07)) and brachial plexus injury (AOR = 6.21 (95% CI: 2.22-17.4)), while infants delivered by CS during labor had no increased risk for these complications, as compared to VD.
Conclusion: While rates of neonatal complications after VE are generally low, higher odds ratios for intra- and extracranial hemorrhages and brachial plexus injuries after VE, compared with other modes of delivery, support a continued cautious use of VE for preterm delivery.
Figures
Similar articles
-
Vacuum assisted birth and risk for cerebral complications in term newborn infants: a population-based cohort study.BMC Pregnancy Childbirth. 2014 Jan 20;14:36. doi: 10.1186/1471-2393-14-36. BMC Pregnancy Childbirth. 2014. PMID: 24444326 Free PMC article.
-
Vacuum extraction in fetal macrosomia and risk of neonatal complications: a population-based cohort study.Acta Obstet Gynecol Scand. 2016 Oct;95(10):1089-96. doi: 10.1111/aogs.12952. Acta Obstet Gynecol Scand. 2016. PMID: 27472147
-
Vaginal breech delivery at term and neonatal morbidity and mortality - a population-based cohort study in Sweden.J Matern Fetal Neonatal Med. 2019 Jan;32(2):265-270. doi: 10.1080/14767058.2017.1378328. Epub 2017 Sep 22. J Matern Fetal Neonatal Med. 2019. PMID: 28889774
-
Neonatal complications among 596 infants delivered by vacuum extraction (in relation to characteristics of the extraction).J Matern Fetal Neonatal Med. 2018 Sep;31(18):2402-2408. doi: 10.1080/14767058.2017.1344631. Epub 2017 Jul 10. J Matern Fetal Neonatal Med. 2018. PMID: 28629251
-
Cesarean section on request at 39 weeks: impact on shoulder dystocia, fetal trauma, neonatal encephalopathy, and intrauterine fetal demise.Semin Perinatol. 2006 Oct;30(5):276-87. doi: 10.1053/j.semperi.2006.07.009. Semin Perinatol. 2006. PMID: 17011400 Review.
Cited by
-
Prevention and Therapy of Preterm Birth. Guideline of the DGGG, OEGGG and SGGG (S2k Level, AWMF Registry Number 015/025, September 2022) - Part 2 with Recommendations on the Tertiary Prevention of Preterm Birth and on the Management of Preterm Premature Rupture of Membranes.Geburtshilfe Frauenheilkd. 2023 May 4;83(5):569-601. doi: 10.1055/a-2044-0345. eCollection 2023 May. Geburtshilfe Frauenheilkd. 2023. PMID: 37169014 Free PMC article.
-
Clinical assessment of the infant and child following perinatal brachial plexus injury.J Hand Ther. 2015 Apr-Jun;28(2):126-33; quiz 134. doi: 10.1016/j.jht.2015.01.001. Epub 2015 Jan 16. J Hand Ther. 2015. PMID: 25840493 Free PMC article. Review.
-
Head Injuries Related to Birth Trauma in Low Birthweight Neonates During Vacuum Extraction.Geburtshilfe Frauenheilkd. 2023 Jan 19;83(2):201-211. doi: 10.1055/a-1987-5765. eCollection 2023 Feb. Geburtshilfe Frauenheilkd. 2023. PMID: 36908698 Free PMC article.
-
Prevention and Therapy of Preterm Birth. Guideline of the DGGG, OEGGG and SGGG (S2k Level, AWMF Registry Number 015/025, February 2019) - Part 2 with Recommendations on the Tertiary Prevention of Preterm Birth and the Management of Preterm Premature Rupture of Membranes.Geburtshilfe Frauenheilkd. 2019 Aug;79(8):813-833. doi: 10.1055/a-0903-2735. Epub 2019 Aug 12. Geburtshilfe Frauenheilkd. 2019. PMID: 31423017 Free PMC article.
-
Neurodevelopmental Outcome at Corrected Age of 2 Years among Children Born Preterm with Operative Vaginal Delivery: A Population-Based Study (LIFT Cohort).J Clin Med. 2023 Jul 28;12(15):4970. doi: 10.3390/jcm12154970. J Clin Med. 2023. PMID: 37568372 Free PMC article.
References
-
- Blencove H, Cousens S, Oestergaard M, Chou D, Moller A-B, Narwal R, Adler A, Garcia CV, Rohde S, Say L, Lawn JE. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379:2162–72. doi: 10.1016/S0140-6736(12)60820-4. - DOI - PubMed
-
- Drife J. Mode of delivery in the early pretern infant (<28 weeks) BJOG. 2006;113(3):81–85. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
