

Off-hour presentation and outcomes in patients with acute myocardial infarction: systematic review and meta-analysis
- PMID: 24452368
- PMCID: PMC3898160
- DOI: 10.1136/bmj.f7393
Off-hour presentation and outcomes in patients with acute myocardial infarction: systematic review and meta-analysis
Abstract
Objective: To assess the association between off-hour (weekends and nights) presentation, door to balloon times, and mortality in patients with acute myocardial infarction.
Data sources: Medline in-process and other non-indexed citations, Medline, Embase, Cochrane Database of Systematic Reviews, and Scopus through April 2013.
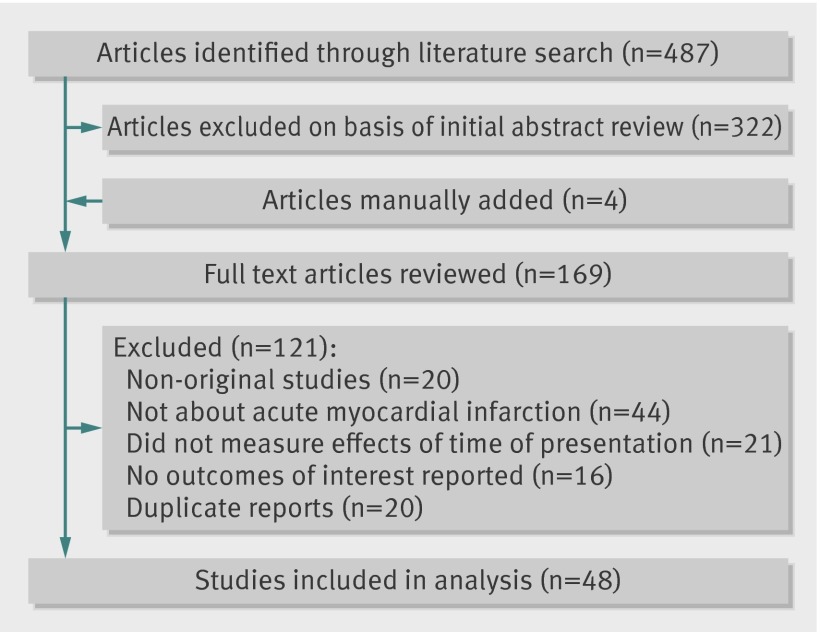
Study selection: Any study that evaluated the association between time of presentation to a healthcare facility and mortality or door to balloon times among patients with acute myocardial infarction was included.
Data extraction: Studies' characteristics and outcomes data were extracted. Quality of studies was assessed with the Newcastle-Ottawa scale. A random effect meta-analysis model was applied. Heterogeneity was assessed using the Q statistic and I(2).
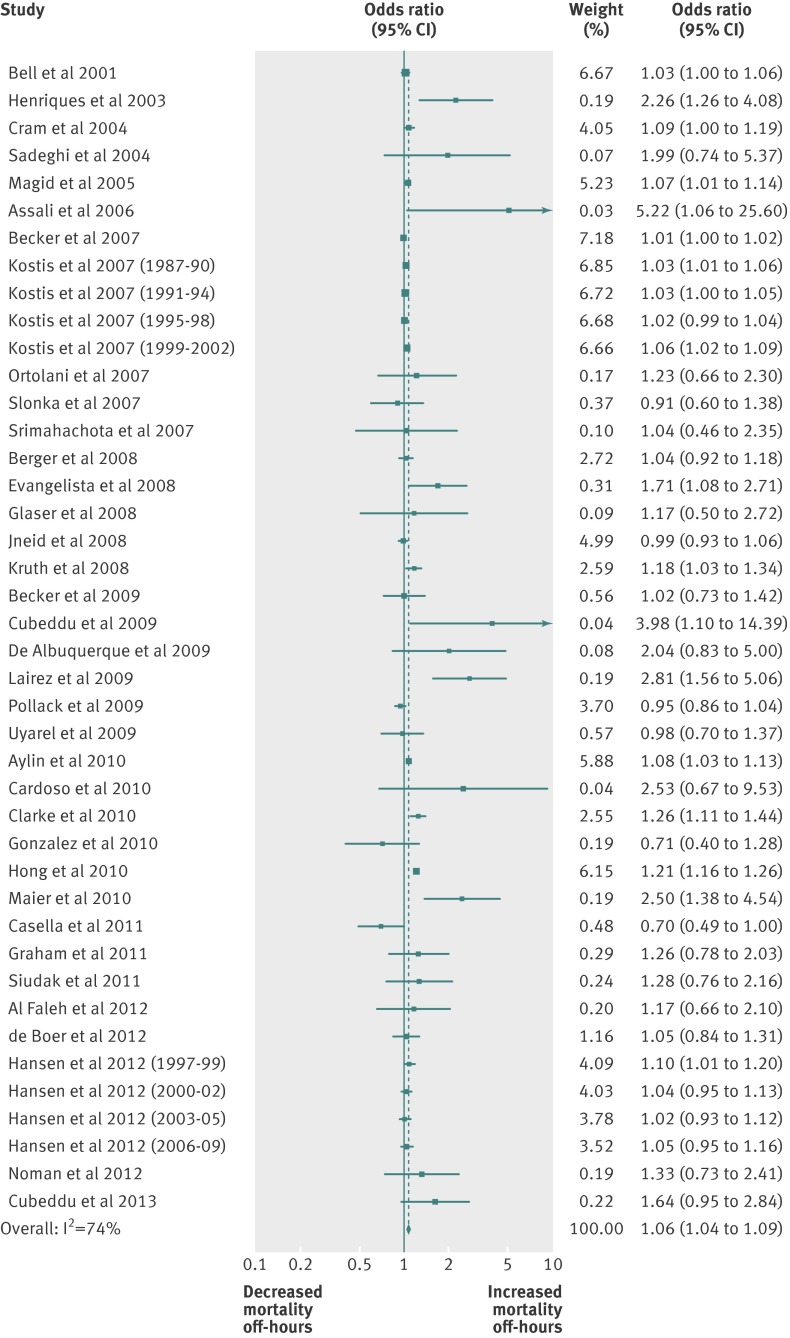
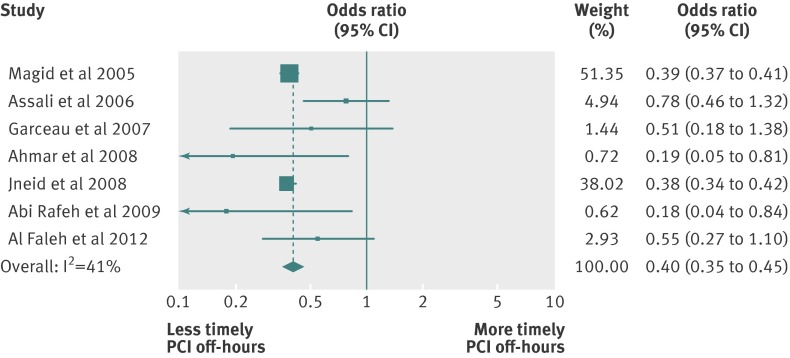
Results: 48 studies with fair quality, enrolling 1,896,859 patients, were included in the meta-analysis. 36 studies reported mortality outcomes for 1,892,424 patients with acute myocardial infarction, and 30 studies reported door to balloon times for 70,534 patients with ST elevation myocardial infarction (STEMI). Off-hour presentation for patients with acute myocardial infarction was associated with higher short term mortality (odds ratio 1.06, 95% confidence interval 1.04 to 1.09). Patients with STEMI presenting during off-hours were less likely to receive percutaneous coronary intervention within 90 minutes (odds ratio 0.40, 0.35 to 0.45) and had longer door to balloon time by 14.8 (95% confidence interval 10.7 to 19.0) minutes. A diagnosis of STEMI and countries outside North America were associated with larger increase in mortality during off-hours. Differences in mortality between off-hours and regular hours have increased in recent years. Analyses were associated with statistical heterogeneity.
Conclusion: This systematic review suggests that patients with acute myocardial infarction presenting during off-hours have higher mortality, and patients with STEMI have longer door to balloon times. Clinical performance measures may need to account for differences arising from time of presentation to a healthcare facility.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Acute myocardial infarction.BMJ. 2014 Jan 21;348:f7696. doi: 10.1136/bmj.f7696. BMJ. 2014. PMID: 24452407 No abstract available.
-
Associations and clinical significance in meta-analysis: when are the deductions too presumptive?J R Coll Physicians Edinb. 2014;44(2):131-2. doi: 10.4997/JRCPE.2014.209. J R Coll Physicians Edinb. 2014. PMID: 24999775 No abstract available.
References
-
- Clarke MS, Wills RA, Bowman RV, Zimmerman PV, Fong KM, Coory MD, et al. Exploratory study of the ‘weekend effect’ for acute medical admissions to public hospitals in Queensland, Australia. Intern Med J 2010;40:777-83. - PubMed
-
- Kostis WJ, Demissie K, Marcella SW, Shao YH, Wilson AC, Moreyra AE. Weekend versus weekday admission and mortality from myocardial infarction. N Engl J Med 2007;356:1099-109. - PubMed
-
- Kruth P, Zeymer U, Gitt A, Junger C, Wienbergen H, Niedermeier F, et al. Influence of presentation at the weekend on treatment and outcome in ST-elevation myocardial infarction in hospitals with catheterization laboratories. Clin Res Cardiol 2008;97:742-7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous