

Population pharmacokinetic modelling of recombinant factor IX Fc fusion protein (rFIXFc) in patients with haemophilia B
- PMID: 24452809
- PMCID: PMC3997831
- DOI: 10.1007/s40262-013-0129-7
Population pharmacokinetic modelling of recombinant factor IX Fc fusion protein (rFIXFc) in patients with haemophilia B
Abstract
Background and objectives: Recombinant factor IX Fc fusion protein (rFIXFc) is a clotting factor developed using monomeric Fc fusion technology to prolong the circulating half-life of factor IX. The objective of this analysis was to elucidate the pharmacokinetic characteristics of rFIXFc in patients with haemophilia B and identify covariates that affect rFIXFc disposition.
Methods: Population pharmacokinetic analysis using NONMEM(®) was performed with clinical data from two completed trials in previously treated patients with severe to moderate haemophilia B. Twelve patients from a phase 1/2a study and 123 patients from a registrational phase 3 study were included in this population analysis.
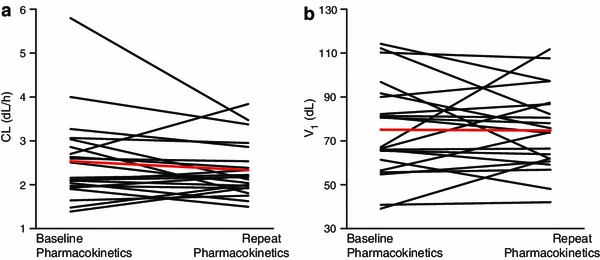
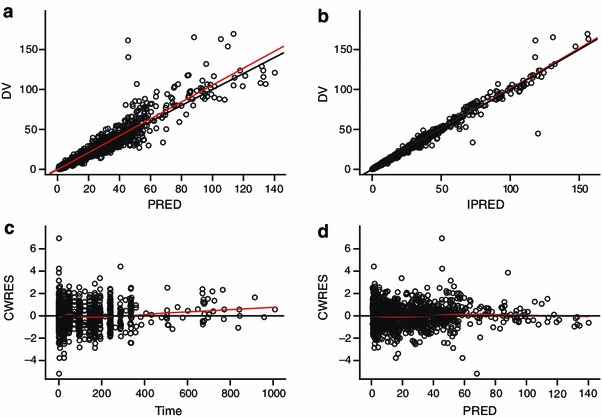
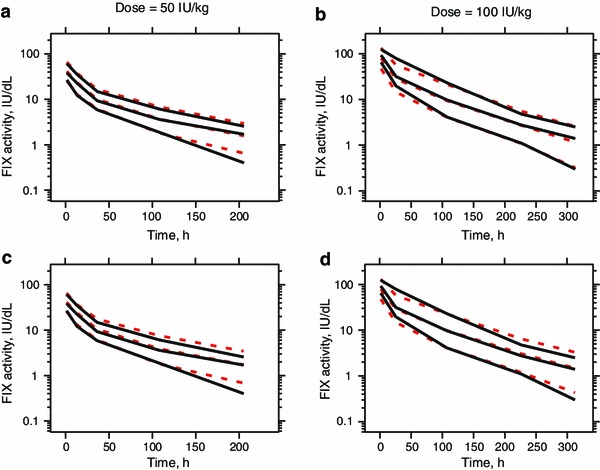
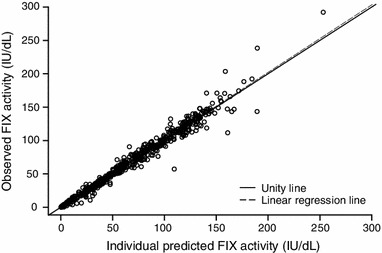
Results: A three-compartment model was found to best describe the pharmacokinetics of rFIXFc. For a typical 73 kg patient, the clearance (CL), volume of the central compartment (V 1) and volume of distribution at steady state (V ss) were 2.39 dL/h, 71.4 dL and 198 dL, respectively. Because of repeat pharmacokinetic profiles at week 26 for patients in a subgroup, inclusion of inter-occasion variability (IOV) on CL and V 1 were evaluated and significantly improved the model. The magnitude of IOV on CL and V 1 were both low to moderate (<20 %) and less than the corresponding inter-individual variability. Body weight (BW) was found to be the only significant covariate for rFIXFc disposition. However, the impact of BW was limited, as the BW power exponents on CL and V 1 were 0.436 and 0.396, respectively.
Conclusion: This is the first population pharmacokinetic analysis that systematically characterized the pharmacokinetics of long-lasting rFIXFc in patients with haemophilia B. The population pharmacokinetic model for rFIXFc can be utilized to evaluate and optimize dosing regimens for the treatment of patients with haemophilia B.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
