

Quality of care for patients with acute coronary syndromes as a function of hospital revascularization capability: Insights from get with the guidelines-CAD
- PMID: 24452828
- PMCID: PMC6649649
- DOI: 10.1002/clc.22246
Quality of care for patients with acute coronary syndromes as a function of hospital revascularization capability: Insights from get with the guidelines-CAD
Abstract
Background: Revascularization availability at US hospitals varies and may impact care quality for acute coronary syndrome patients.
Hypothesis: The hypothesis of this study was that there would be differences in care quality at Get With The Guidelines-Coronary Artery Disease (GWTG-CAD) hospitals based on revascularization capability.
Methods: For acute coronary syndrome patients admitted to GWTG-CAD hospitals between 2000 and 2010, care quality at hospitals with or without revascularization capability was examined by assessing conformity with performance and quality measures.
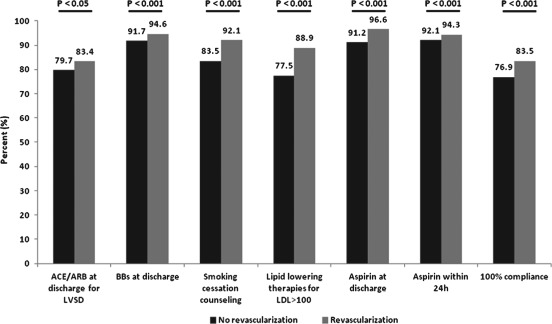
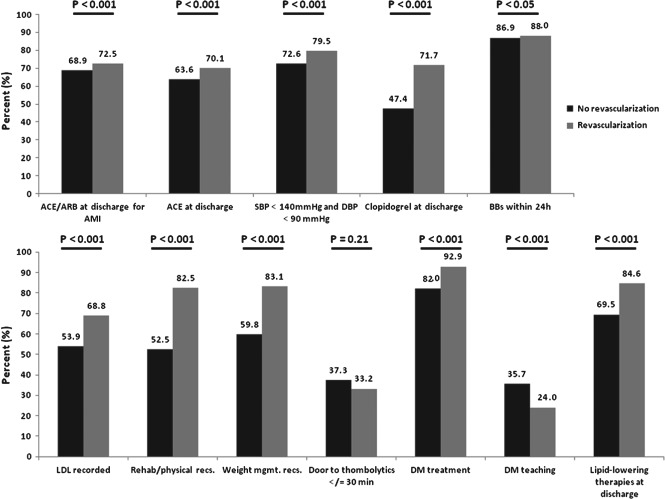
Results: This study included 95 999 acute coronary syndrome patients admitted to 310 GWTG-CAD hospitals. There were 89 000 patients admitted to 226 revascularization-capable hospitals and 6999 patients admitted to 84 hospitals without revascularization capability included. Adjusted multivariate analysis demonstrated that 8 of the 19 measures were more frequently performed in the revascularization cohort: aspirin (odds ratio [OR]: 1.41, 95% confidence interval [CI]: 1.04-1.92), clopidogrel (OR: 2.31, 95% CI: 1.78-3.00), lipid-lowering therapies at discharge (OR: 1.39, 95% CI: 1.04-1.87), lipid-lowering therapies for low-density lipoprotein >100 mg/dL (OR: 1.85, 95% CI: 1.23-2.77), achievement of blood pressure <140/90 mm Hg (OR: 1.20, 95% CI: 1.03-1.40), LDL recorded (OR: 1.47, 95% CI: 1.05-2.06), and recommendations offered for physical activity (OR: 3.82, 95% CI: 2.23-6.55) or weight management (OR: 1.74, 95% CI: 1.12-2.69).
Conclusions: The GWTG-CAD revascularization hospitals were associated with better performance in some, but not all, measures assessed. Although the difference in conformity between hospital types was modest for performance measures but more variable for quality measures, room for improvement exists in key aspects of care.
© 2014 Wiley Periodicals, Inc.
Figures
References
-
- Patel MR, Chen AY, Roe MT, et al. A comparison of acute coronary syndrome care at academic and nonacademic hospitals. Am J Med. 2007;120:40–46. - PubMed
-
- Roe MT, Chen AY, Delong ER, et al. Patterns of transfer for patients with non‐ST‐segment elevation acute coronary syndrome from community to tertiary care hospitals. Am Heart J. 2008;156:185–192. - PubMed
-
- Hiratzka LF, Eagle KA, Liang L, et al; Get With The Guidelines Steering Committee . Atherosclerosis secondary prevention performance measures after coronary bypass graft surgery compared with percutaneous catheter intervention and nonintervention patients in the Get With The Guidelines Database. Circulation. 2007;116(11 suppl):I207–I212. - PubMed
-
- LaBresh KA, Ellrodt AG, Gliklich R, et al. Get With The Guidelines for cardiovascular secondary prevention: pilot results. Arch Intern Med. 2004;164:203–209. - PubMed
-
- LaBresh KA, Fonarow GC, Smith SC Jr, et al; Get With The Guidelines Steering Committee . Improved treatment of hospitalized coronary artery disease patients with the Get With The Guidelines program. Crit Pathw Cardiol. 2007;6:98–105. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
