

Bone marrow mesenchymal stromal cells to treat tissue damage in allogeneic stem cell transplant recipients: correlation of biological markers with clinical responses
- PMID: 24452962
- PMCID: PMC3991733
- DOI: 10.1002/stem.1638
Bone marrow mesenchymal stromal cells to treat tissue damage in allogeneic stem cell transplant recipients: correlation of biological markers with clinical responses
Abstract
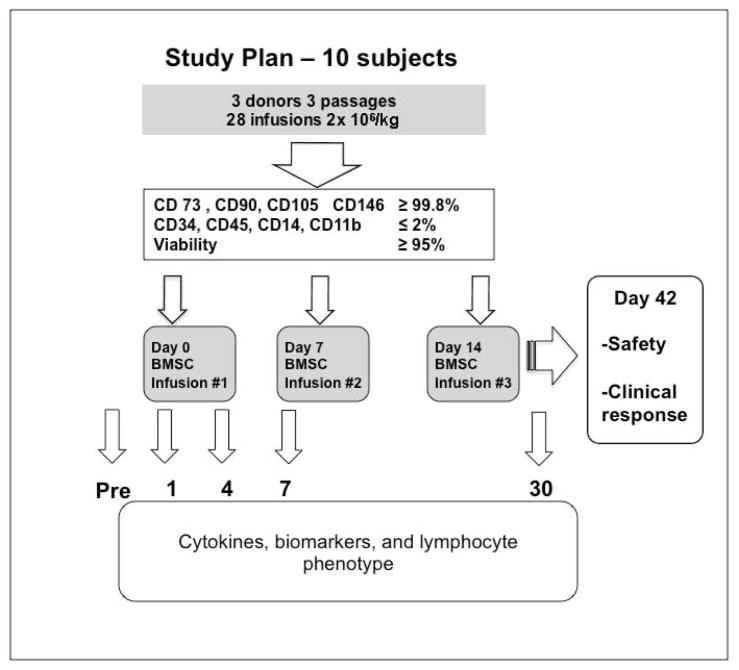
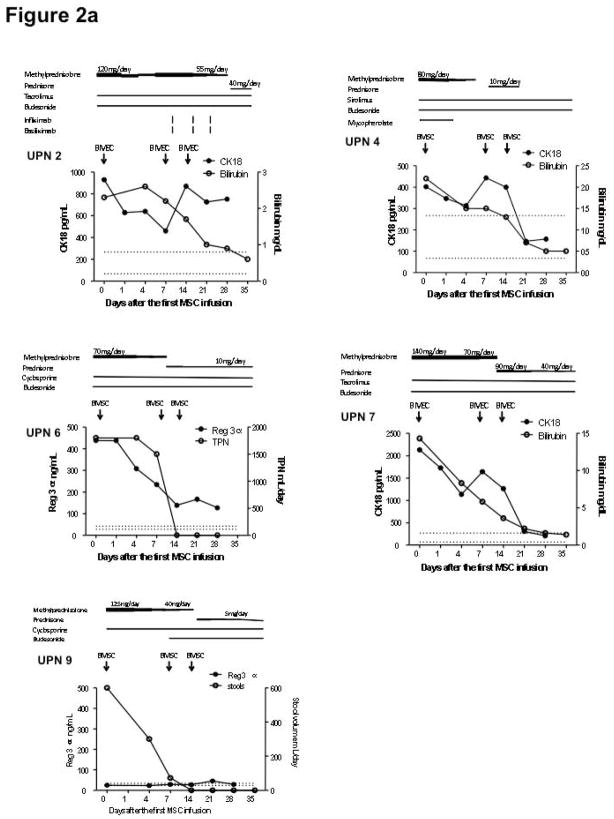
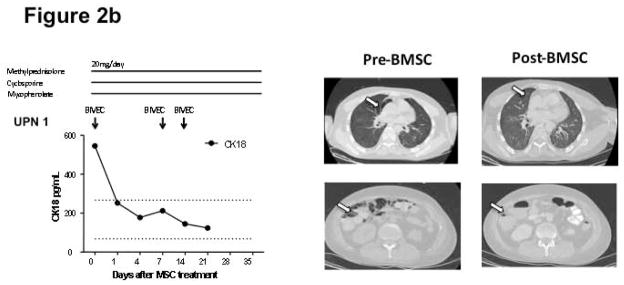
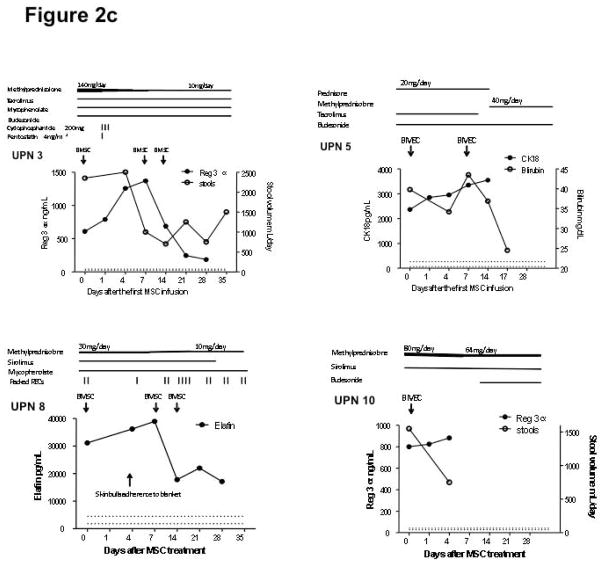
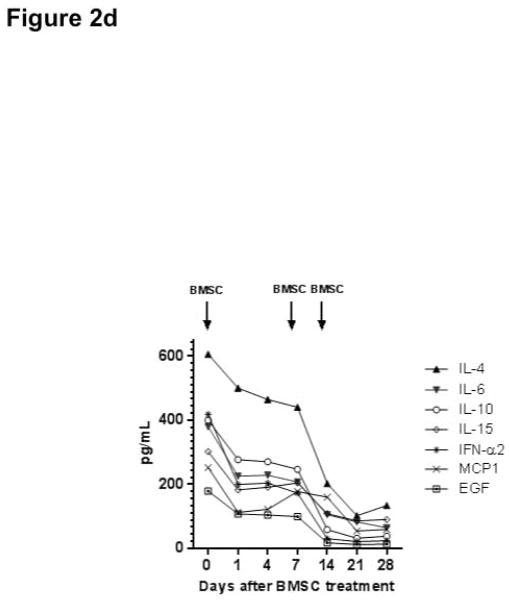
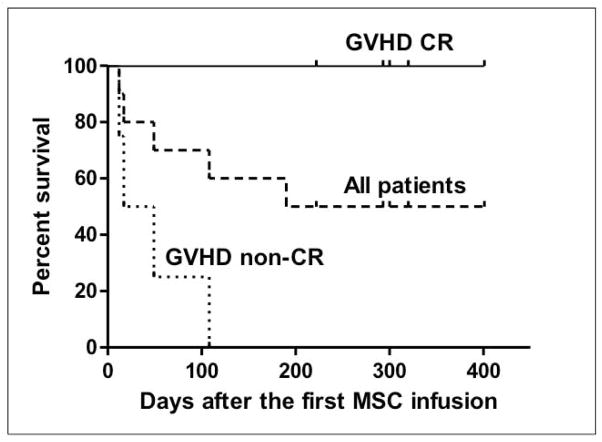
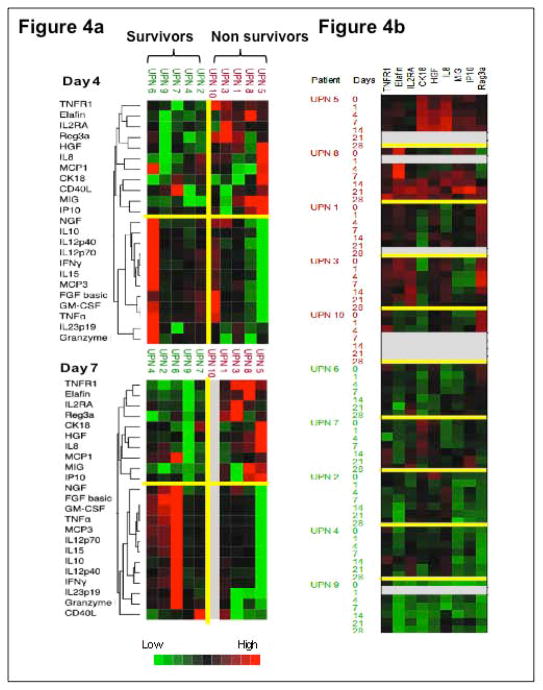
Bone marrow mesenchymal stromal cells (BMSCs) have been used to treat acute graft-versus-host disease (GVHD) and other complications following allogeneic hematopoietic stem cell transplantation (SCT). We conducted a phase I trial using third party, early passage BMSCs for patients with steroid-refractory GVHD, tissue injury, or marrow failure following SCT to investigate safety and efficacy. To identify mechanisms of BMSC immunomodulation and tissue repair, patients were serially monitored for plasma GVHD biomarkers, cytokines, and lymphocyte phenotype. Ten subjects were infused a fixed dose of 2 × 10(6) BMSCs/kg intravenously weekly for three doses. There was no treatment-related toxicity (primary endpoint). Eight subjects were evaluable for response at 4 weeks after the last infusion. Five of the seven patients with steroid-refractory acute GVHD achieved a complete response, two of two patients with tissue injury (pneumomediastinum/pneumothorax) achieved resolution but there was no response in two subjects with delayed marrow failure. Rapid reductions in inflammatory cytokines were observed. Clinical responses correlated with a fall in biomarkers (Reg 3α, CK18, and Elafin) relevant for the site of GVHD or tissue injury. The GVHD complete responders survived significantly longer and had higher baseline absolute lymphocyte and central memory CD4 and CD8 counts. Cytokine changes also segregated with survival. These results confirm that BMSCs are associated with rapid clinical and biomarker responses in GVHD and tissue injury. However, BMSCs were ineffective in patients with prolonged GVHD with lower lymphocyte counts, which suggest that effective GVHD control by BMSCs requires a relatively intact immune system.
Keywords: Allogeneic stem cell transplantation; Biomarkers; Graft-versus-host disease; Mesenchymal stromal cell.
© 2014 AlphaMed Press.
Conflict of interest statement
Figures
References
-
- Jitschin R, Mougiakakos D, Von Bahr L, et al. Alterations in the cellular immune compartment of patients treated with third-party mesenchymal stromal cells following allogeneic hematopoietic stem-cell transplantation. Stem Cells. 2013 - PubMed
-
- Le Blanc K, Frassoni F, Ball L, et al. Mesenchymal stem cells for treatment of steroid-resistant, severe, acute graft-versus-host disease: a phase II study. Lancet. 2008;371:1579–1586. - PubMed
-
- Le Blanc K, Rasmusson I, Sundberg B, et al. Treatment of severe acute graft-versus-host disease with third party haploidentical mesenchymal stem cells. Lancet. 2004;363:1439–1441. - PubMed
-
- Prasad VK, Lucas KG, Kleiner GI, et al. Efficacy and Safety of Ex-vivo Cultured Adult Human Mesenchymal Stem Cells (Prochymal(TM)) in Pediatric Patients with Severe Refractory Acute Graft-Versus-Host Disease in a Compassionate Use study. Biol Blood Marrow Transplant. 2011 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
