

Muscle-strengthening and conditioning activities and risk of type 2 diabetes: a prospective study in two cohorts of US women
- PMID: 24453948
- PMCID: PMC3891575
- DOI: 10.1371/journal.pmed.1001587
Muscle-strengthening and conditioning activities and risk of type 2 diabetes: a prospective study in two cohorts of US women
Abstract
Background: It is well established that aerobic physical activity can lower the risk of type 2 diabetes (T2D), but whether muscle-strengthening activities are beneficial for the prevention of T2D is unclear. This study examined the association of muscle-strengthening activities with the risk of T2D in women.
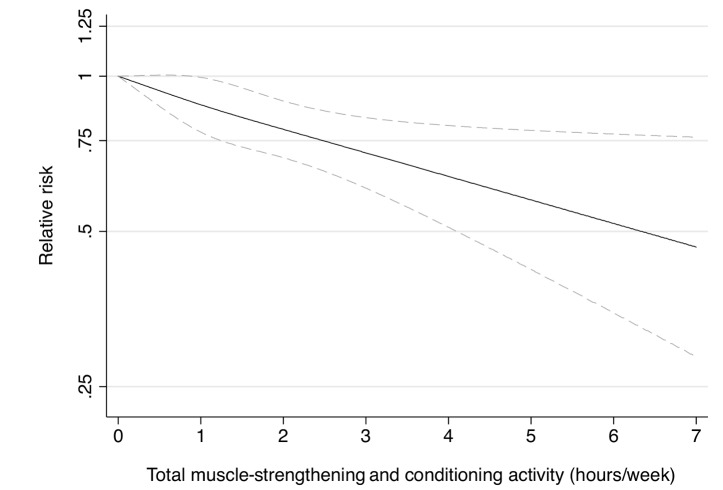
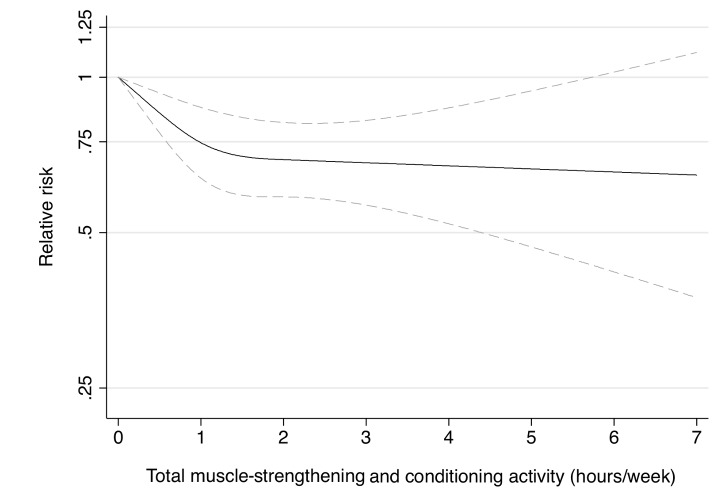
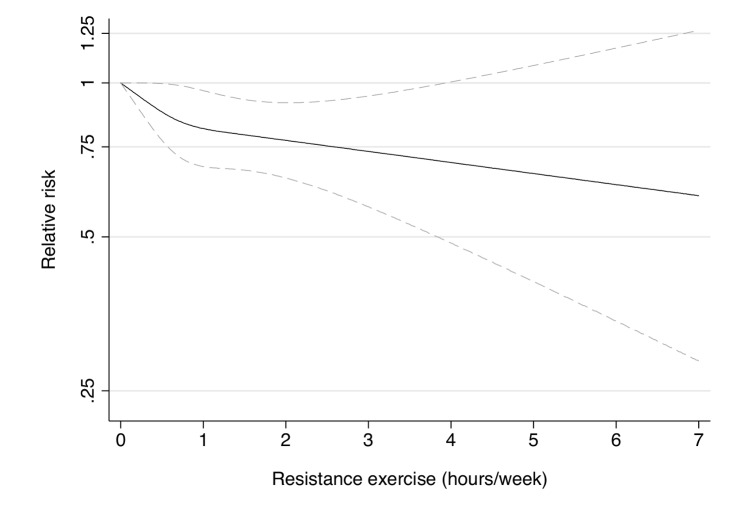
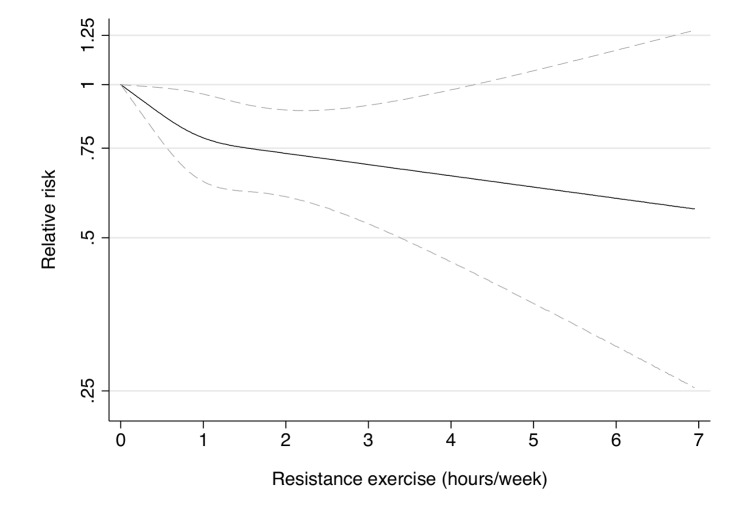
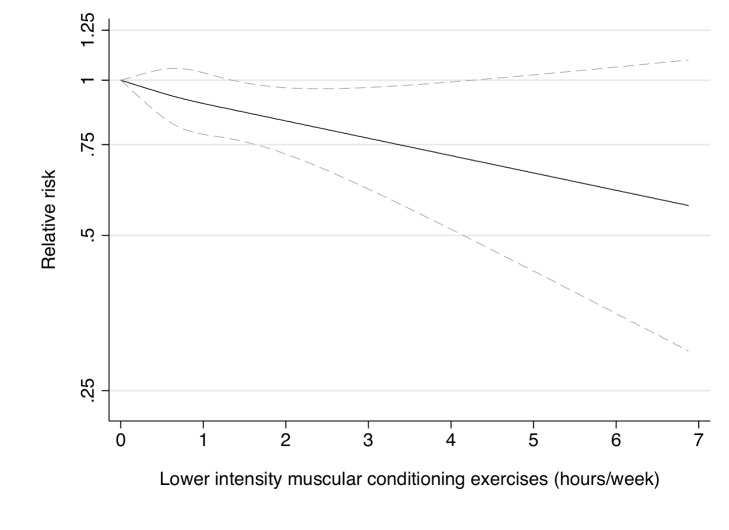
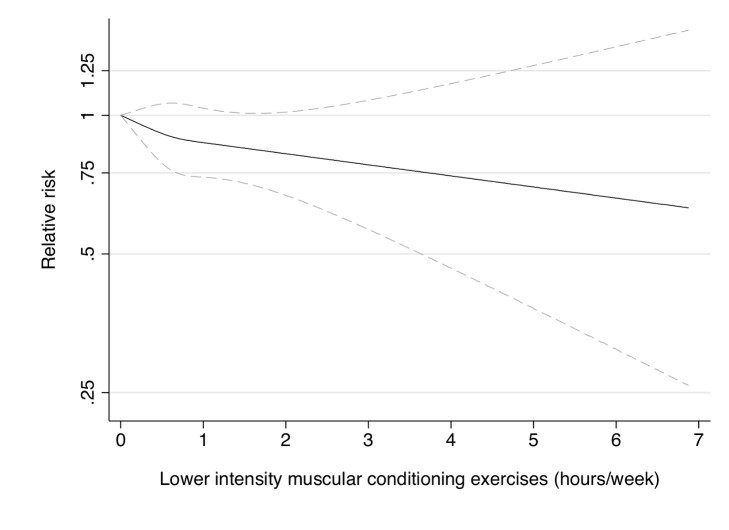
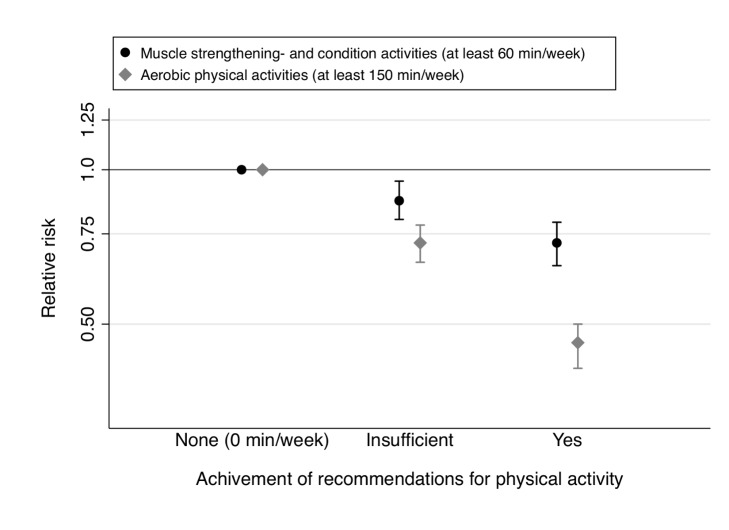
Methods and findings: We prospectively followed up 99,316 middle-aged and older women for 8 years from the Nurses' Health Study ([NHS] aged 53-81 years, 2000-2008) and Nurses' Health Study II ([NHSII] aged 36-55 years, 2001-2009), who were free of diabetes, cancer, and cardiovascular diseases at baseline. Participants reported weekly time spent on resistance exercise, lower intensity muscular conditioning exercises (yoga, stretching, toning), and aerobic moderate and vigorous physical activity (MVPA) at baseline and in 2004/2005. Cox regression with adjustment for major determinants for T2D was carried out to examine the influence of these types of activities on T2D risk. During 705,869 person years of follow-up, 3,491 incident T2D cases were documented. In multivariable adjusted models including aerobic MVPA, the pooled relative risk (RR) for T2D for women performing 1-29, 30-59, 60-150, and >150 min/week of total muscle-strengthening and conditioning activities was 0.83, 0.93, 0.75, and 0.60 compared to women reporting no muscle-strengthening and conditioning activities (p<0.001 for trend). Furthermore, resistance exercise and lower intensity muscular conditioning exercises were each independently associated with lower risk of T2D in pooled analyses. Women who engaged in at least 150 min/week of aerobic MVPA and at least 60 min/week of muscle-strengthening activities had substantial risk reduction compared with inactive women (pooled RR = 0.33 [95% CI 0.29-0.38]). Limitations to the study include that muscle-strengthening and conditioning activity and other types of physical activity were assessed by a self-administered questionnaire and that the study population consisted of registered nurses with mostly European ancestry.
Conclusions: Our study suggests that engagement in muscle-strengthening and conditioning activities (resistance exercise, yoga, stretching, toning) is associated with a lower risk of T2D. Engagement in both aerobic MVPA and muscle-strengthening type activity is associated with a substantial reduction in the risk of T2D in middle-aged and older women.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Hu FB, Leitzmann MF, Stampfer MJ, Colditz GA, Willett WC, et al. (2001) Physical activity and television watching in relation to risk for type 2 diabetes mellitus in men. Arch Intern Med 161: 1542–1548. - PubMed
-
- Hu FB, Li TY, Colditz GA, Willett WC, Manson JE (2003) Television watching and other sedentary behaviors in relation to risk of obesity and type 2 diabetes mellitus in women. JAMA 289: 1785–1791. - PubMed
-
- Sigal RJ, Kenny GP, BoulÇ NG, Wells GA, Prud'homme D, et al. (2007) Effects of aerobic training, resistance training, or both on glycemic control in type 2 diabetes. Ann Intern Med 147: 357–369. - PubMed
-
- Dunstan DW, Daly RM, Owen N, Jolley D, de C, et al. (2002) High-intensity resistance training improves glycemic control in older patients with type 2 diabetes. Diabetes Care 25: 1729–1736. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
