Sarcoidosis mimicking cancer metastasis following chemotherapy for ovarian cancer
- PMID: 24454009
- PMCID: PMC3893334
- DOI: 10.4143/crt.2013.45.4.354
Sarcoidosis mimicking cancer metastasis following chemotherapy for ovarian cancer
Abstract
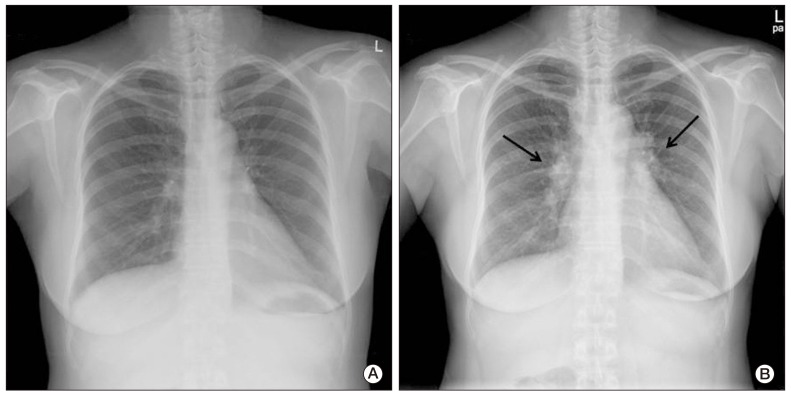
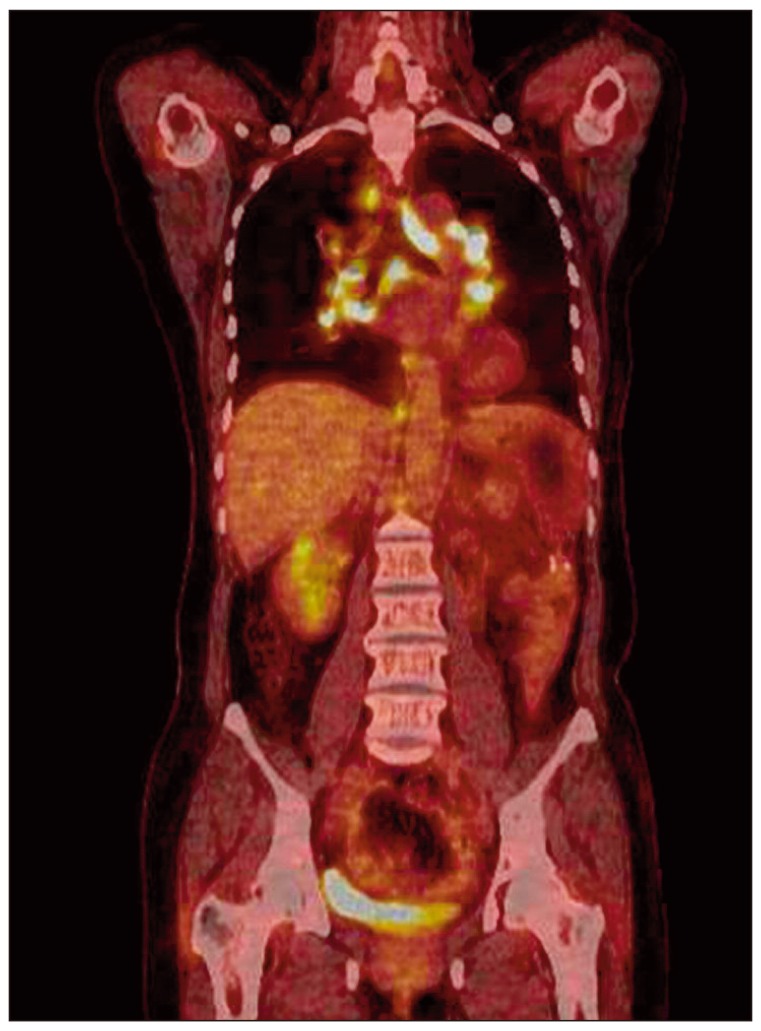
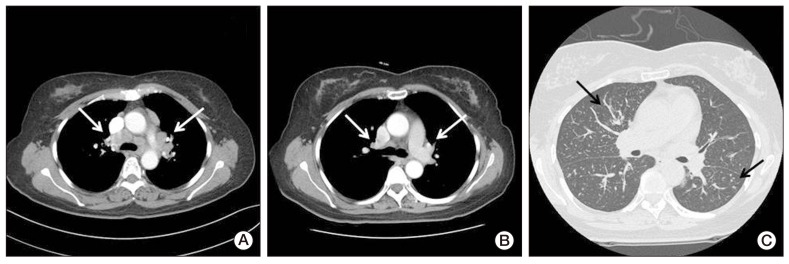
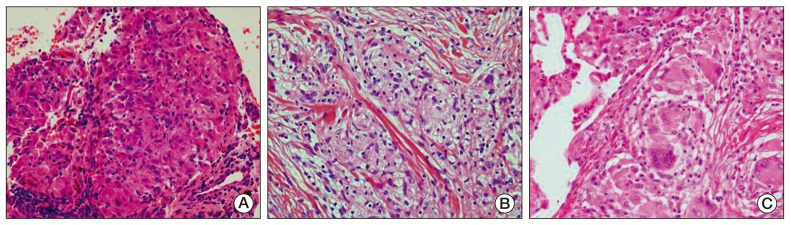
We report on a rare case of sarcoidosis that developed after chemotherapy for ovarian cancer, and mimicked a cancer metastasis. A 52-year-old female diagnosed with stage III ovarian cancer underwent curative surgery and postoperative chemotherapy. Four months later, her whole-body positron emission tomography and computed tomography (CT) scan showed high uptake in the mediastinal lymph nodes, and ovarian cancer recurrence was suspected. Biopsy of the mediastinal lymph nodes and subcutaneous nodules revealed noncaseating granulomas. These lesions resolved spontaneously without treatment; however, newly developed perilymphatic and centrilobular nodules were observed on follow-up chest CT. Surgical biopsy of these lesions also showed noncaseating granulomas. She was finally diagnosed with sarcoidosis.
Keywords: Drug therapy; Ovarian neoplasms; Positron-emission tomography and computed tomography; Sarcoidosis.
Conflict of interest statement
Conflict of interest relevant to this article was not reported.
Figures
Similar articles
-
Sarcoidosis mimicking metastatic thyroid cancer following radioactive iodine therapy.J Community Hosp Intern Med Perspect. 2015 Feb 3;5(1):26360. doi: 10.3402/jchimp.v5.26360. eCollection 2015. J Community Hosp Intern Med Perspect. 2015. PMID: 25656675 Free PMC article.
-
Endometrial Cancer with Sarcoidosis in Regional Lymph Nodes: A Case Report.Case Rep Oncol. 2015 Oct 7;8(3):409-15. doi: 10.1159/000440800. eCollection 2015 Sep-Dec. Case Rep Oncol. 2015. PMID: 26557079 Free PMC article.
-
Sarcoidosis mimicking lymphoma on FDG-PET imaging.Radiol Case Rep. 2015 Nov 6;6(2):409. doi: 10.2484/rcr.v6i2.409. eCollection 2011. Radiol Case Rep. 2015. PMID: 27307894 Free PMC article.
-
[A case of sarcoidosis following chemotherapy for follicular lymphoma].Nihon Kokyuki Gakkai Zasshi. 2010 Oct;48(10):774-8. Nihon Kokyuki Gakkai Zasshi. 2010. PMID: 21066868 Review. Japanese.
-
[A Case of Sarcoidosis Associated with Esophageal Cancer].Gan To Kagaku Ryoho. 2018 Nov;45(11):1649-1652. Gan To Kagaku Ryoho. 2018. PMID: 30449856 Review. Japanese.
Cited by
-
Coexistence of sarcoidosis and metastatic lesions: A diagnostic and therapeutic dilemma.Oncol Lett. 2017 Dec;14(6):7643-7652. doi: 10.3892/ol.2017.7247. Epub 2017 Oct 20. Oncol Lett. 2017. PMID: 29344212 Free PMC article.
-
Subcutaneous sarcoidosis (Darier-Roussy sarcoidosis) with extensive disease on positron emission tomography: A case report and review of the literature.Respirol Case Rep. 2022 Apr 10;10(5):e0949. doi: 10.1002/rcr2.949. eCollection 2022 May. Respirol Case Rep. 2022. PMID: 35433008 Free PMC article.
-
Sarcoid-Like Reaction after Complete Remission of Malignancy: CT and 18F-FDG PET/CT Features for the Differential Diagnosis from Lymph Node Metastasis.Taehan Yongsang Uihakhoe Chi. 2021 Jul;82(4):903-913. doi: 10.3348/jksr.2020.0091. Epub 2020 Dec 23. Taehan Yongsang Uihakhoe Chi. 2021. PMID: 36238067 Free PMC article.
-
A case of endobronchial metastasis of colon cancer mimics sarcoidosis, and a review of related literature.J Cancer Res Clin Oncol. 2023 Nov;149(16):15287-15292. doi: 10.1007/s00432-023-05214-y. Epub 2023 Aug 18. J Cancer Res Clin Oncol. 2023. PMID: 37594535 Free PMC article. Review.
-
Sarcoidosis Occurring After Solid Cancer: A Nonfortuitous Association: Report of 12 Cases and Review of the Literature.Medicine (Baltimore). 2015 Jul;94(28):e928. doi: 10.1097/MD.0000000000000928. Medicine (Baltimore). 2015. PMID: 26181571 Free PMC article. Review.
References
-
- Newman LS, Rose CS, Maier LA. Sarcoidosis. N Engl J Med. 1997;336:1224–1234. - PubMed
-
- Caras WE, Dillard T, Baker T, Pluss J. Coexistence of sarcoidosis and malignancy. South Med J. 2003;96:918–922. - PubMed
-
- Reich JM, Mullooly JP, Johnson RE. Linkage analysis of malignancy-associated sarcoidosis. Chest. 1995;107:605–613. - PubMed
-
- Brincker H. Sarcoid reactions in malignant tumours. Cancer Treat Rev. 1986;13:147–156. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources