

Maternal mortality in India: causes and healthcare service use based on a nationally representative survey
- PMID: 24454701
- PMCID: PMC3893075
- DOI: 10.1371/journal.pone.0083331
Maternal mortality in India: causes and healthcare service use based on a nationally representative survey
Abstract
Background: Data on cause-specific mortality, skilled birth attendance, and emergency obstetric care access are essential to plan maternity services. We present the distribution of India's 2001-2003 maternal mortality by cause and uptake of emergency obstetric care, in poorer and richer states.
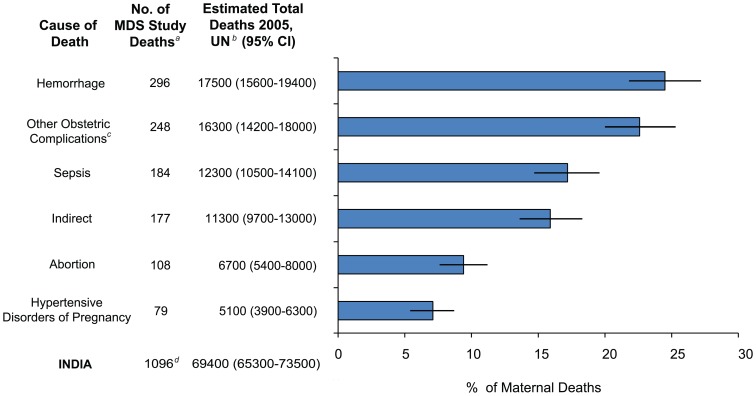
Methods and findings: The Registrar General of India surveyed all deaths occurring in 2001-2003 in 1.1 million nationally representative homes. Field staff interviewed household members about events that preceded the death. Two physicians independently assigned a cause of death. Narratives for all maternal deaths were coded for variables on healthcare uptake. Distribution of number of maternal deaths, cause-specific mortality and uptake of healthcare indicators were compared for poorer and richer states. There were 10,041 all-cause deaths in women age 15-49 years, of which 1096 (11.1%) were maternal deaths. Based on 2004-2006 SRS national MMR estimates of 254 deaths per 100,000 live births, we estimated rural areas of poorer states had the highest MMR (397, 95%CI 385-410) compared to the lowest MMR in urban areas of richer states (115, 95%CI 85-146). We estimated 69,400 maternal deaths in India in 2005. Three-quarters of maternal deaths were clustered in rural areas of poorer states, although these regions have only half the estimated live births in India. Most maternal deaths were attributed to direct obstetric causes (82%). There was no difference in the major causes of maternal deaths between poorer and richer states. Two-thirds of women died seeking some form of healthcare, most seeking care in a critical medical condition. Rural areas of poorer states had proportionately lower access and utilization to healthcare services than the urban areas; however this rural-urban difference was not seen in richer states.
Conclusions: Maternal mortality and poor access to healthcare is disproportionately higher in rural populations of the poorer states of India.
Conflict of interest statement
Figures



References
-
- RGI (2006) Registrar General/Centre for Global Health Research, University of Toronto. New Delhi: Registrar General of India.
-
- WHO, UNICEF, UNFPA, World Bank (2012) Trends in maternal mortality: 1990 to 2010. Geneva: World Health Organization.
-
- IIPS (2010) District level household and facility survey (DLHS-3) 2007–2008: India. Mumbai: International Institute for Population Sciences.
-
- Barros AJD, Ronsmans C, Axelson H, Loaiza E, Bertoldi AD, et al. (2012) Equity in maternal, newborn, and child health interventions in countdown to 2015: a retrospective review of survey data from 54 countries. Lancet 379: 1225–1233. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
