

Deficient EBV-specific B- and T-cell response in patients with chronic fatigue syndrome
- PMID: 24454857
- PMCID: PMC3893202
- DOI: 10.1371/journal.pone.0085387
Deficient EBV-specific B- and T-cell response in patients with chronic fatigue syndrome
Abstract
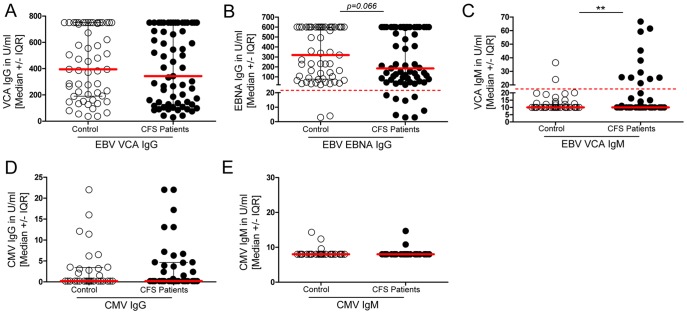
Epstein-Barr virus (EBV) has long been discussed as a possible cause or trigger of Chronic Fatigue Syndrome (CFS). In a subset of patients the disease starts with infectious mononucleosis and both enhanced and diminished EBV-specific antibody titers have been reported. In this study, we comprehensively analyzed the EBV-specific memory B- and T-cell response in patients with CFS. While we observed no difference in viral capsid antigen (VCA)-IgG antibodies, EBV nuclear antigen (EBNA)-IgG titers were low or absent in 10% of CFS patients. Remarkably, when analyzing the EBV-specific memory B-cell reservoir in vitro a diminished or absent number of EBNA-1- and VCA-antibody secreting cells was found in up to 76% of patients. Moreover, the ex vivo EBV-induced secretion of TNF-α and IFN-γ was significantly lower in patients. Multicolor flow cytometry revealed that the frequencies of EBNA-1-specific triple TNF-α/IFN-γ/IL-2 producing CD4(+) and CD8(+) T-cell subsets were significantly diminished whereas no difference could be detected for HCMV-specific T-cell responses. When comparing EBV load in blood immune cells, we found more frequently EBER-DNA but not BZLF-1 RNA in CFS patients compared to healthy controls suggesting more frequent latent replication. Taken together, our findings give evidence for a deficient EBV-specific B- and T-cell memory response in CFS patients and suggest an impaired ability to control early steps of EBV reactivation. In addition the diminished EBV response might be suitable to develop diagnostic marker in CFS.
Conflict of interest statement
Figures





Similar articles
-
Serological profiling of the EBV immune response in Chronic Fatigue Syndrome using a peptide microarray.PLoS One. 2017 Jun 12;12(6):e0179124. doi: 10.1371/journal.pone.0179124. eCollection 2017. PLoS One. 2017. PMID: 28604802 Free PMC article.
-
IgM serum antibodies to Epstein-Barr virus are uniquely present in a subset of patients with the chronic fatigue syndrome.In Vivo. 2004 Mar-Apr;18(2):101-6. In Vivo. 2004. PMID: 15113035
-
Increased T-cell responses to Epstein-Barr virus with high viral load in patients with Epstein-Barr virus-positive diffuse large B-cell lymphoma.Leuk Lymphoma. 2015 Apr;56(4):1072-8. doi: 10.3109/10428194.2014.938326. Epub 2014 Aug 13. Leuk Lymphoma. 2015. PMID: 24975317
-
Epstein-Barr Virus and the Origin of Myalgic Encephalomyelitis or Chronic Fatigue Syndrome.Front Immunol. 2021 Nov 15;12:656797. doi: 10.3389/fimmu.2021.656797. eCollection 2021. Front Immunol. 2021. PMID: 34867935 Free PMC article. Review.
-
Serologic and virologic epidemiology of Epstein-Barr virus: relevance to chronic fatigue syndrome.Rev Infect Dis. 1991 Jan-Feb;13 Suppl 1:S19-25. doi: 10.1093/clinids/13.supplement_1.s19. Rev Infect Dis. 1991. PMID: 1850540 Review.
Cited by
-
Chronic viral infections in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS).J Transl Med. 2018 Oct 1;16(1):268. doi: 10.1186/s12967-018-1644-y. J Transl Med. 2018. PMID: 30285773 Free PMC article. Review.
-
Different risk factors distinguish myalgic encephalomyelitis/chronic fatigue syndrome from severe fatigue.Sci Rep. 2023 Feb 11;13(1):2469. doi: 10.1038/s41598-023-29329-x. Sci Rep. 2023. PMID: 36774379 Free PMC article.
-
EBV/HHV-6A dUTPases contribute to myalgic encephalomyelitis/chronic fatigue syndrome pathophysiology by enhancing TFH cell differentiation and extrafollicular activities.JCI Insight. 2022 Jun 8;7(11):e158193. doi: 10.1172/jci.insight.158193. JCI Insight. 2022. PMID: 35482424 Free PMC article.
-
Pharmaceutical Interventions in Chronic Fatigue Syndrome: A Literature-based Commentary.Clin Ther. 2019 May;41(5):798-805. doi: 10.1016/j.clinthera.2019.02.011. Epub 2019 Mar 11. Clin Ther. 2019. PMID: 30871727 Free PMC article.
-
Effects of Chronic Diurnal Disruption and Acute Inflammatory Challenge on Mice with Latent Murine Gammaherpesvirus Infection.Comp Med. 2016 Dec 1;66(6):445-454. Comp Med. 2016. PMID: 28304247 Free PMC article.
References
-
- Christley Y, Duffy T, Martin CR (2012) A review of the definitional criteria for chronic fatigue syndrome. J Eval Clin Pract 18: 25–31. - PubMed
-
- Fukuda K, Straus SE, Hickie I, Sharpe MC, Dobbins JG, et al. (1994) The chronic fatigue syndrome: a comprehensive approach to its definition and study. International Chronic Fatigue Syndrome Study Group. Ann Intern Med 121: 953–959. - PubMed
-
- Tanaka Y (2012) Biomarkers of stress and fatigue. Nihon Rinsho 70: 880–886. - PubMed
-
- Bansal AS, Bradley AS, Bishop KN, Kiani-Alikhan S, Ford B (2012) Chronic fatigue syndrome, the immune system and viral infection. Brain Behav Immun 26: 24–31. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
