

Positron emission tomography-computed tomography in the management of lung cancer: An update
- PMID: 24455612
- PMCID: PMC3892522
- DOI: 10.4103/2278-330X.114148
Positron emission tomography-computed tomography in the management of lung cancer: An update
Abstract
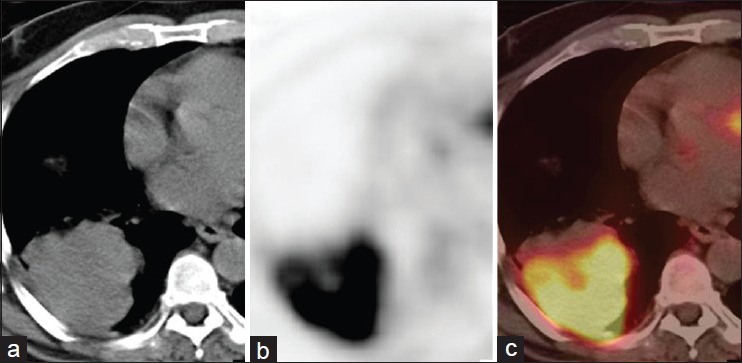
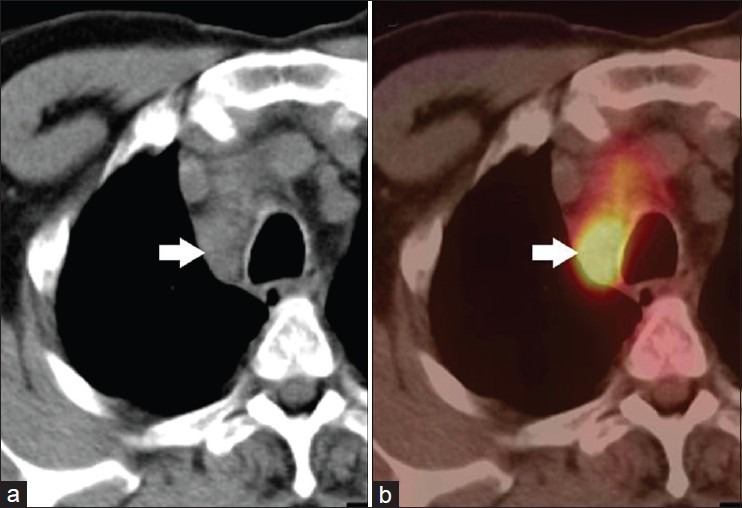
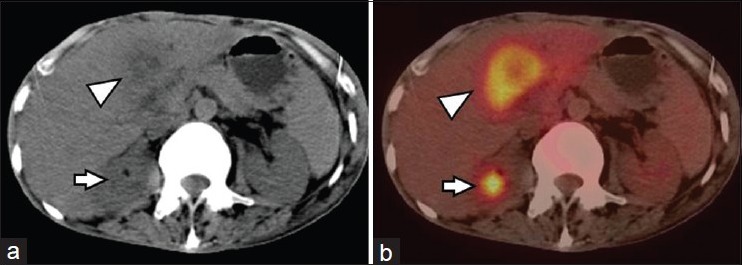
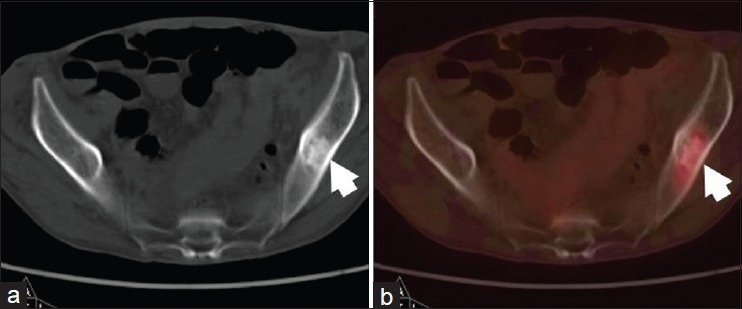
This communication presents an update on the current role of positron emission tomography-computed tomography (PET-CT) in the various clinical decision-making steps in lung carcinoma. The modality has been reported to be useful in characterizing solitary pulmonary nodules, improving lung cancer staging, especially for the detection of nodal and metastatic site involvement, guiding therapy, monitoring treatment response, and predicting outcome in non-small cell lung carcinoma (NSCLC). Its role has been more extensively evaluated in NSCLC than small cell lung carcinoma (SCLC). Limitations in FDG PET-CT are encountered in cases of tumor histotypes characterized by low glucose uptake (mucinous forms, bronchioalveolar carcinoma, neuroendocrine tumors), in the assessment of brain metastases (high physiologic 18F-FDG uptake in the brain) and in cases presenting with associated inflammation. The future potentials of newer PET tracers beyond FDG are enumerated. An evolving area is PET-guided assessment of targeted therapy (e.g., EGFR and EGFR tyrosine kinase overexpression) in tumors which have significant potential for drug development.
Keywords: Lung cancer; PET-CT; restaging; solitary pulmonary nodule; staging.
Conflict of interest statement
Figures
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–49. - PubMed
-
- Sant M, Allemani C, Santaquilani M, Knijn A, Marchesi F, Capocaccia R EUROCARE Working Group. EUROCARE-4. Survival of cancer patients diagnosed in 1995-1999. Results and commentary. Eur J Cancer. 2009;45:931–91. - PubMed
-
- Brennan P, Hainaut P, Boffetta P. Genetics of lung-cancer susceptibility. Lancet Oncol. 2011;12:399–408. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
