

Lung protection during non-invasive synchronized assist versus volume control in rabbits
- PMID: 24456613
- PMCID: PMC4057206
- DOI: 10.1186/cc13706
Lung protection during non-invasive synchronized assist versus volume control in rabbits
Abstract
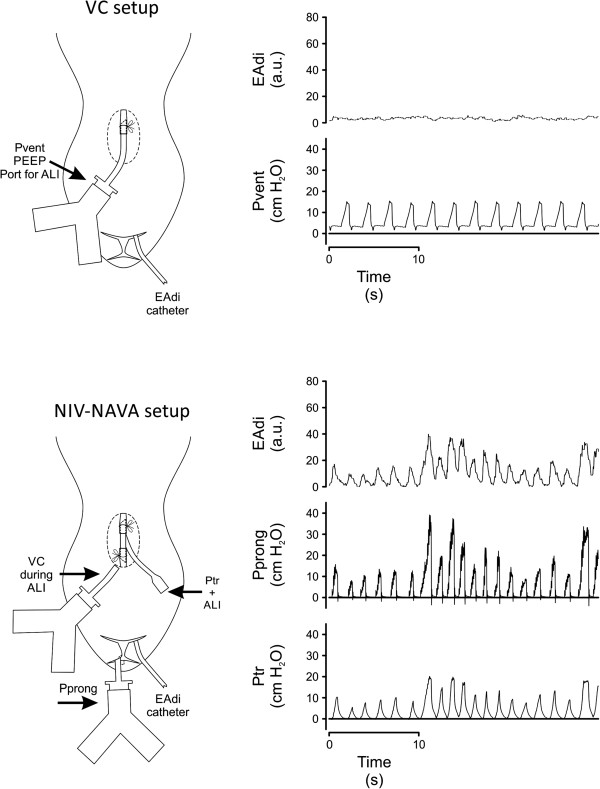
Introduction: Experimental work provides insight into potential lung protective strategies. The objective of this study was to evaluate markers of ventilator-induced lung injury after two different ventilation approaches: (1) a "conventional" lung-protective strategy (volume control (VC) with low tidal volume, positive end-expiratory pressure (PEEP) and paralysis), (2) a physiological approach with spontaneous breathing, permitting synchrony, variability and a liberated airway. For this, we used non-invasive Neurally Adjusted Ventilatory Assist (NIV-NAVA), with the hypothesis that liberation of upper airways and the ventilator's integration with lung protective reflexes would be equally lung protective.
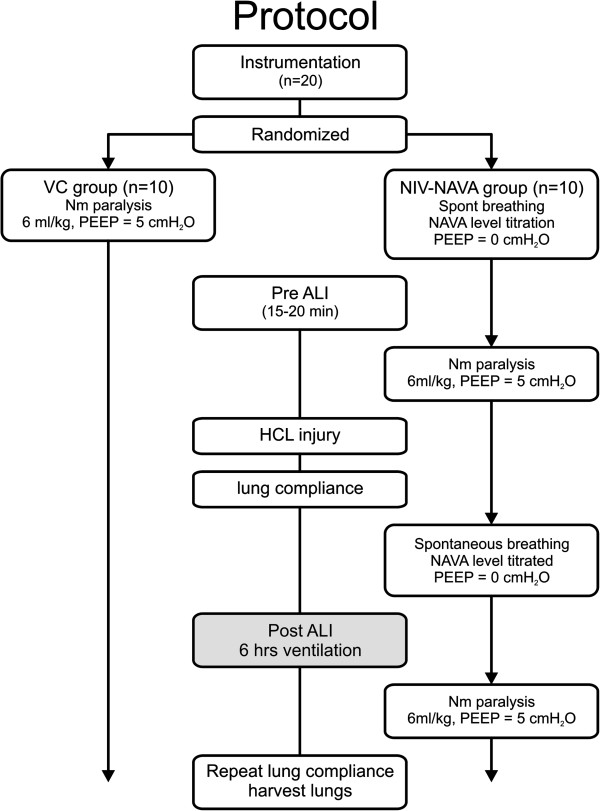
Methods: In this controlled and randomized in vivo laboratory study, 25 adult White New Zealand rabbits were studied, including five non-ventilated control animals. The twenty animals with aspiration-induced lung injury were randomized to ventilation with either VC (6 mL/kg, PEEP 5 cm H2O, and paralysis) or NIV-NAVA for six hours (PEEP = zero because of leaks). Markers of lung function, lung injury, vital signs and ventilator parameters were assessed.
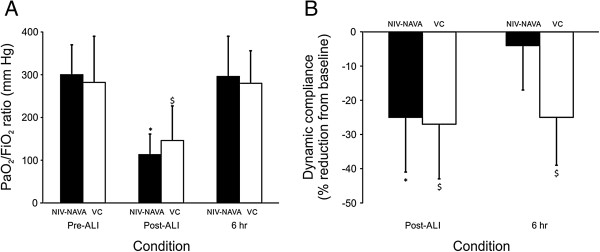
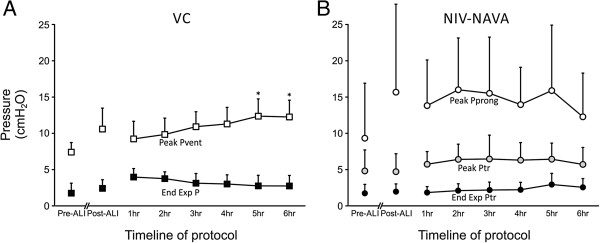
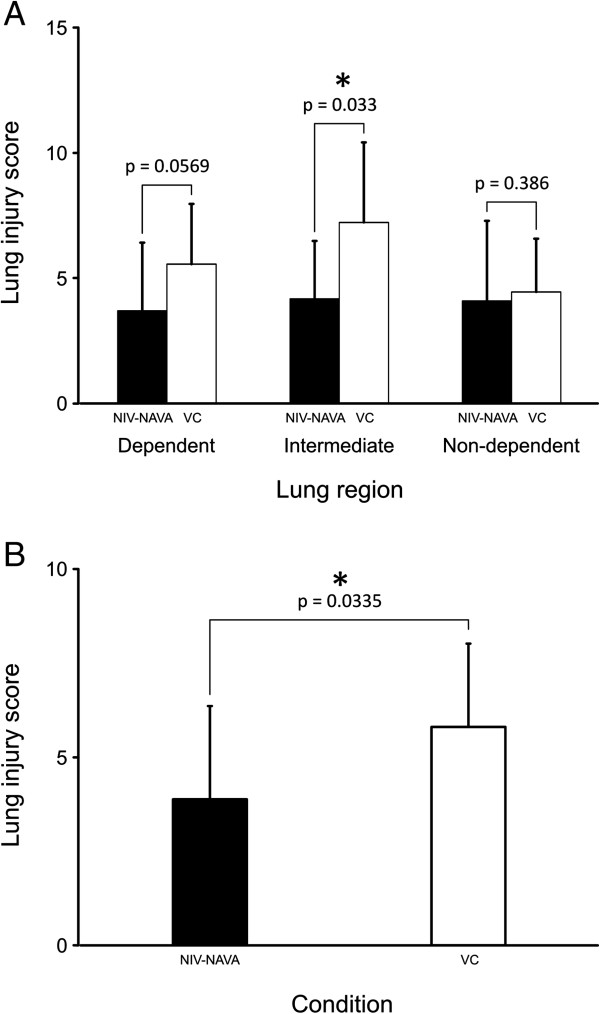
Results: At the end of six hours of ventilation (n = 20), there were no significant differences between VC and NIV-NAVA for vital signs, PaO2/FiO2 ratio, lung wet-to-dry ratio and broncho-alveolar Interleukin 8 (Il-8). Plasma IL-8 was higher in VC (P <0.05). Lung injury score was lower for NIV-NAVA (P = 0.03). Dynamic lung compliance recovered after six hours in NIV-NAVA but not in VC (P <0.05). During VC, peak pressures increased from 9.2 ± 2.4 cm H2O (hour 1) to 12.3 ± 12.3 cm H2O (hour 6) (P <0.05). During NIV-NAVA, the tracheal end-expiratory pressure was similar to the end-expiratory pressure during VC. Two animals regurgitated during NIV-NAVA, without clinical consequences, and survived the protocol.
Conclusions: In experimental acute lung injury, NIV-NAVA is as lung-protective as VC 6 ml/kg with PEEP.
Figures


Comment in
-
Another brick in the wall of needs for invasive ventilation?Crit Care. 2014 Mar 17;18(2):122. doi: 10.1186/cc13769. Crit Care. 2014. PMID: 25029382 Free PMC article.
Similar articles
-
Neurally adjusted ventilatory assist decreases ventilator-induced lung injury and non-pulmonary organ dysfunction in rabbits with acute lung injury.Intensive Care Med. 2009 Nov;35(11):1979-89. doi: 10.1007/s00134-009-1626-x. Intensive Care Med. 2009. PMID: 19760209
-
Feasibility of neurally adjusted positive end-expiratory pressure in rabbits with early experimental lung injury.BMC Anesthesiol. 2015 Sep 14;15:124. doi: 10.1186/s12871-015-0103-z. BMC Anesthesiol. 2015. PMID: 26369672 Free PMC article.
-
Influence of neurally adjusted ventilatory assist and positive end-expiratory pressure on breathing pattern in rabbits with acute lung injury.Crit Care Med. 2006 Dec;34(12):2997-3004. doi: 10.1097/01.CCM.0000242520.50665.9F. Crit Care Med. 2006. PMID: 16957635
-
Neurally adjusted ventilatory assist: a ventilation tool or a ventilation toy?Respir Care. 2011 Mar;56(3):327-35. doi: 10.4187/respcare.00775. Epub 2011 Jan 21. Respir Care. 2011. PMID: 21255496 Review.
-
Ventilator-associated lung injury during assisted mechanical ventilation.Semin Respir Crit Care Med. 2014 Aug;35(4):409-17. doi: 10.1055/s-0034-1382153. Epub 2014 Aug 8. Semin Respir Crit Care Med. 2014. PMID: 25105820 Review.
Cited by
-
Another brick in the wall of needs for invasive ventilation?Crit Care. 2014 Mar 17;18(2):122. doi: 10.1186/cc13769. Crit Care. 2014. PMID: 25029382 Free PMC article.
-
Ibuprofen protects ventilator-induced lung injury by downregulating Rho-kinase activity in rats.Biomed Res Int. 2014;2014:749097. doi: 10.1155/2014/749097. Epub 2014 Jun 12. Biomed Res Int. 2014. PMID: 25019086 Free PMC article.
-
Diaphragm-triggered non-invasive respiratory support in preterm infants.Cochrane Database Syst Rev. 2020 Mar 17;3(3):CD012935. doi: 10.1002/14651858.CD012935.pub2. Cochrane Database Syst Rev. 2020. PMID: 32176939 Free PMC article.
-
Non-invasive Respiratory Support of the Premature Neonate: From Physics to Bench to Practice.Front Pediatr. 2020 May 8;8:214. doi: 10.3389/fped.2020.00214. eCollection 2020. Front Pediatr. 2020. PMID: 32457860 Free PMC article. Review.
References
-
- Imai Y, Parodo J, Kajikawa O, de Perrot M, Fischer S, Edwards V, Cutz E, Liu M, Keshavjee S, Martin TR, Marshall JC, Ranieri VM, Slutsky AS. Injurious mechanical ventilation and end-organ epithelial cell apoptosis and organ dysfunction in an experimental model of acute respiratory distress syndrome. JAMA. 2003;289:2104–2112. doi: 10.1001/jama.289.16.2104. - DOI - PubMed
-
- Brander L, Sinderby C, Lecomte F, Leong-Poi H, Bell D, Beck J, Tsoporis JN, Vaschetto R, Schultz MJ, Parker TG, Villar J, Zhang H, Slutsky AS. Neurally adjusted ventilatory assist decreases ventilator-induced lung injury and non-pulmonary organ dysfunction in rabbits with acute lung injury. Intensive Care Med. 2009;35:1979–1989. doi: 10.1007/s00134-009-1626-x. - DOI - PubMed
-
- Yoshida T, Uchiyama A, Matsuura N, Mashimo T, Fujino Y. Spontaneous breathing during lung-protective ventilation in an experimental acute lung injury model: high transpulmonary pressure associated with strong spontaneous breathing effort may worsen lung injury. Crit Care Med. 2012;40:1578–1585. doi: 10.1097/CCM.0b013e3182451c40. - DOI - PubMed
-
- Kuiper JW, Plötz FB, Groeneveld AJ, Haitsma JJ, Jothy S, Vaschetto R, Zhang H, Slutsky AS. High tidal volume mechanical ventilation-induced lung injury in rats is greater after acid instillation than after sepsis-induced acute lung injury, but does not increase systemic inflammation: an experimental study. BMC Anesthesiol. 2011;11:26. doi: 10.1186/1471-2253-11-26. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
