

Maternal vitamin D status and the risk of mild and severe preeclampsia
- PMID: 24457526
- PMCID: PMC4053531
- DOI: 10.1097/EDE.0000000000000039
Maternal vitamin D status and the risk of mild and severe preeclampsia
Abstract
Background: We sought to determine the association between maternal vitamin D status at ≤26 weeks' gestation and the risk of preeclampsia by clinical subtype.
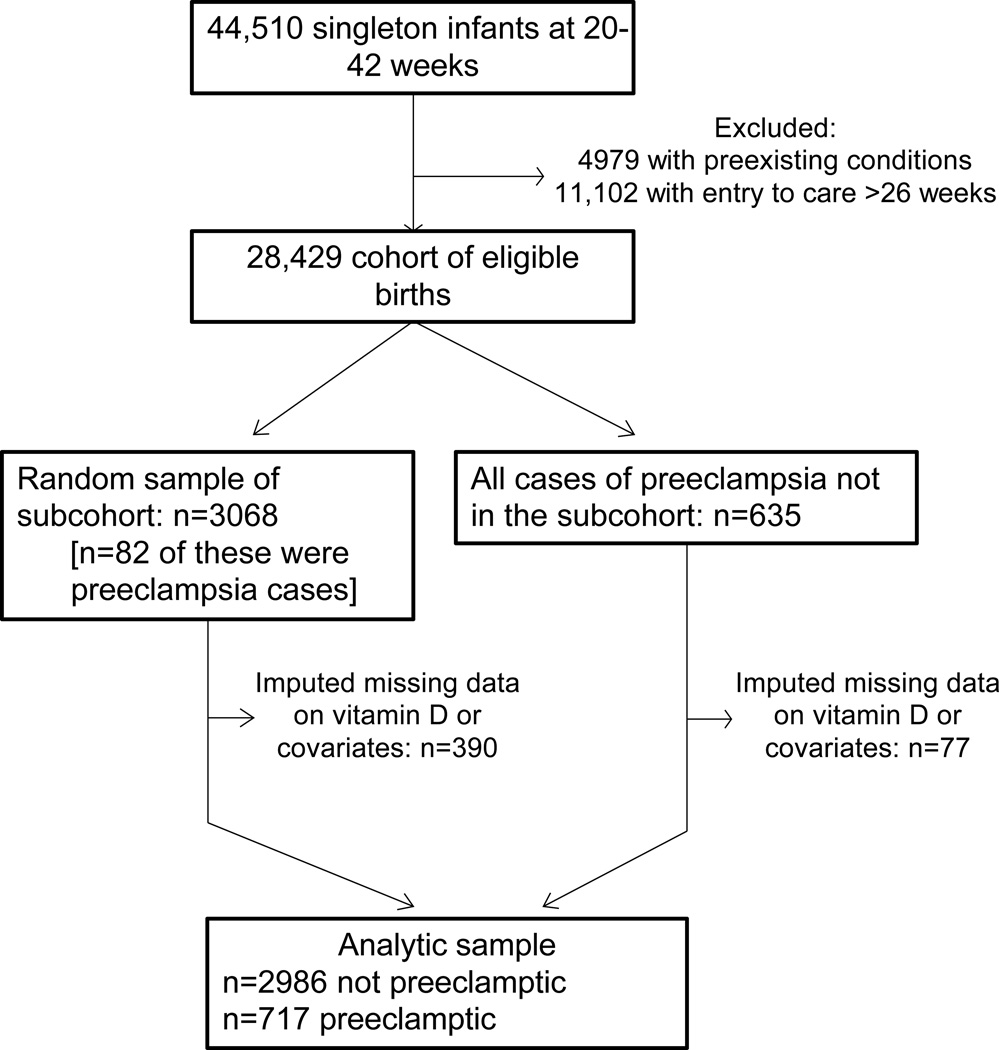
Methods: We conducted a case-cohort study among women enrolled at 12 US sites from 1959 to 1966 in the Collaborative Perinatal Project. In serum collected at ≤26 weeks' gestation (median 20.9 weeks) from 717 women who later developed preeclampsia (560 mild and 157 severe cases) and from 2986 mothers without preeclampsia, we measured serum 25-hydroxyvitamin D, over 40 years later, using liquid chromatography-tandem mass spectrometry.
Results: Half of women in the subcohort had 25-hydroxyvitamin D (25(OH)D) >50 nmol/L. Maternal 25(OH)D 50 to 74.9 nmol/L was associated with a reduction in the absolute and relative risk of preeclampsia and mild preeclampsia compared with 25(OH)D <30 nmol/L in the crude analysis but not after adjustment for confounders, including race, prepregnancy body mass index, and parity. For severe preeclampsia, 25(OH)D ≥50 nmol/L was associated with a reduction in three cases per 1000 pregnancies (adjusted risk difference = -0.003 [95% confidence interval = -0.005 to 0.0002]) and a 40% reduction in risk (0.65 [0.43 to 0.98]) compared with 25(OH)D <50 nmol/L. Conclusions were unchanged (1) after restricting to women with 25(OH)D measured before 22 weeks' gestation or (2) with formal sensitivity analyses for unmeasured confounding.
Conclusions: Maternal vitamin D deficiency may be a risk factor for severe preeclampsia but not for its mild subtypes. Contemporary cohorts with large numbers of severe preeclampsia cases would be needed to confirm or refute these findings.
References
-
- Roberts JM. Pregnancy related hypertension. In: Creasy RK, Resnik R, editors. Maternal Fetal Medicine. Philadelphia: W.B. Saunders; 1998. pp. 883–872.
-
- Goldenberg RL, Rouse DJ. Prevention of premature birth. N Engl J Med. 1998;339(5):313–320. - PubMed
-
- Diagnosis and management of preeclampsia and eclampsia. ACOG Practice Bulletin No. 33. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2002;99:159–167. - PubMed
-
- Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266–281. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
