

Management of liver trauma in Kuwait
- PMID: 24457986
- PMCID: PMC5586862
- DOI: 10.1159/000358126
Management of liver trauma in Kuwait
Abstract
Objectives: The aim of this study was to introduce the concept of non-operative management (NOM) for blunt liver trauma by establishing a protocol and a prospective Liver Trauma Registry in Kuwait.
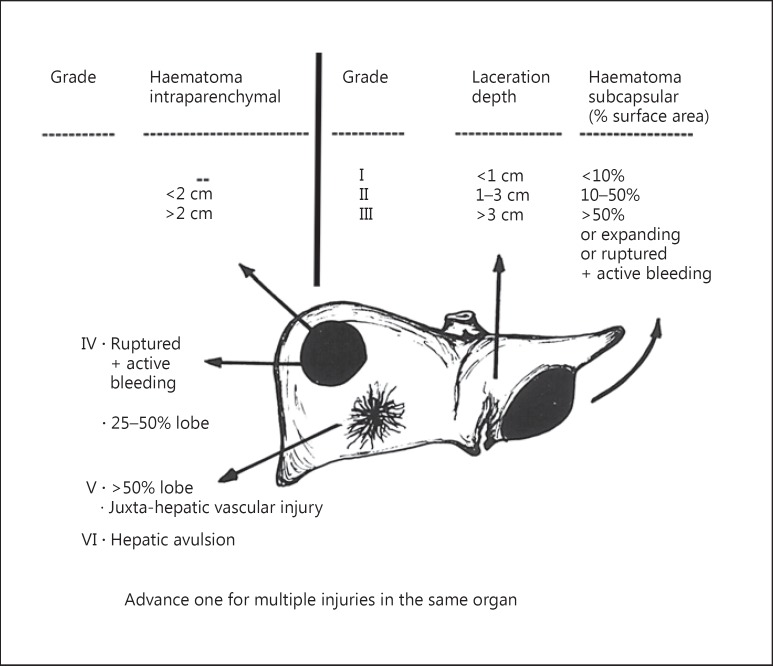
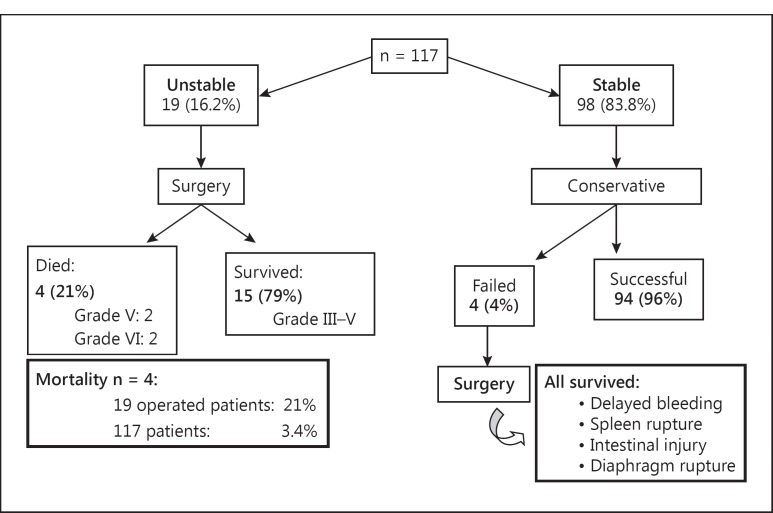
Subjects and methods: A prospective Liver Trauma Registry was started in 4 hospitals and it included 117 patients who had sustained blunt liver trauma (94 men and 23 women). Unstable patients were taken to surgery while stable patients were managed conservatively regardless of the grade of liver injury. High-grade (III-VI) liver injuries were managed in collaboration with the liver surgery specialist.
Results: The mean age of the 117 patients was 29.02 ± 11.18 years (range 7-63). NOM was successful in 94 (96%) patients and failed in 4 (4%) (these 4 then underwent successful surgery). Nineteen (16.2%) were unstable and underwent surgery immediately; 15 (79%) of them survived (they had had grade III-V injuries) and 4 died (2 with grade V injuries and 2 with grade VI injuries). Perihepatic packing was necessary in 8/19 (42%) patients. The overall mortality was 3.4% (4/117).
Conclusions: This study showed that NOM was successful in a majority of patients with blunt liver trauma. In addition, it confirmed that the magnitude of liver injury and haemoperitoneum did not preclude NOM as long as the patient was haemodynamically stable.
© 2014 S. Karger AG, Basel.
Figures
References
-
- Kozar RA, Moore FA, Moore EE, et al. Western Trauma Association critical decisions in trauma: nonoperative management of adult blunt hepatic trauma. J Trauma. 2009;67:1144–1149. - PubMed
-
- Velmahos GC, Toutouzas KG, Radin R, et al. Nonoperative treatment of blunt injury to solid abdominal organs. A prospective study. Arch Surg. 2003;138:844–851. - PubMed
-
- Moore EE, Cogbill TH, Jurkovich GJ, et al. Organ injury scaling: spleen and liver (1994 revision) J Trauma. 1995;38:323–324. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
