

Purse-string morphology of external anal sphincter revealed by novel imaging techniques
- PMID: 24458022
- PMCID: PMC3949029
- DOI: 10.1152/ajpgi.00338.2013
Purse-string morphology of external anal sphincter revealed by novel imaging techniques
Abstract
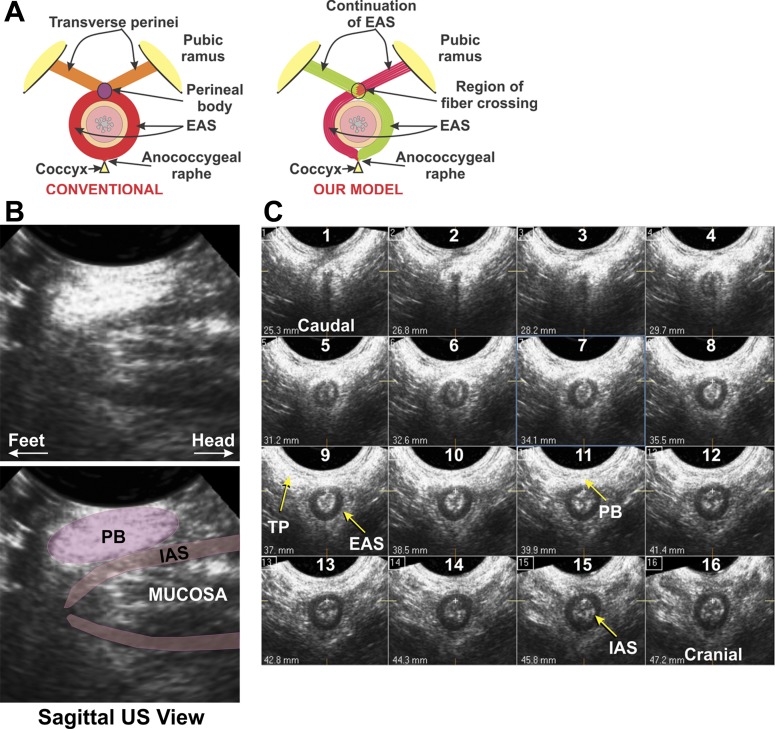
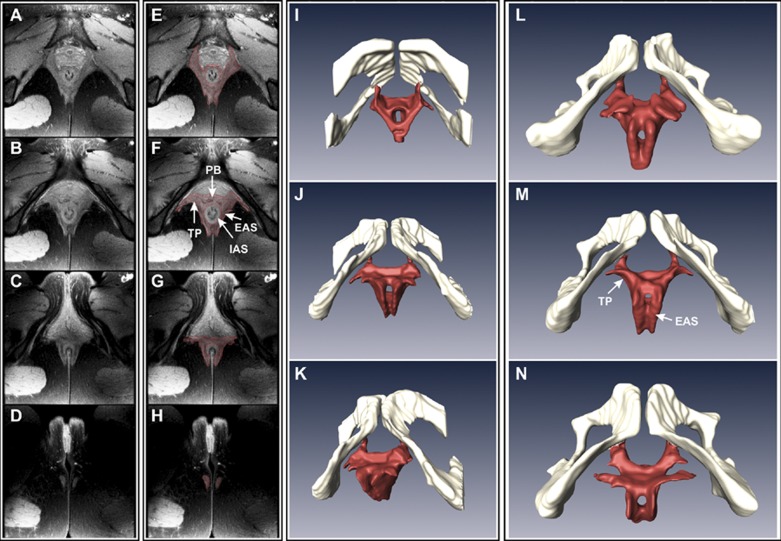
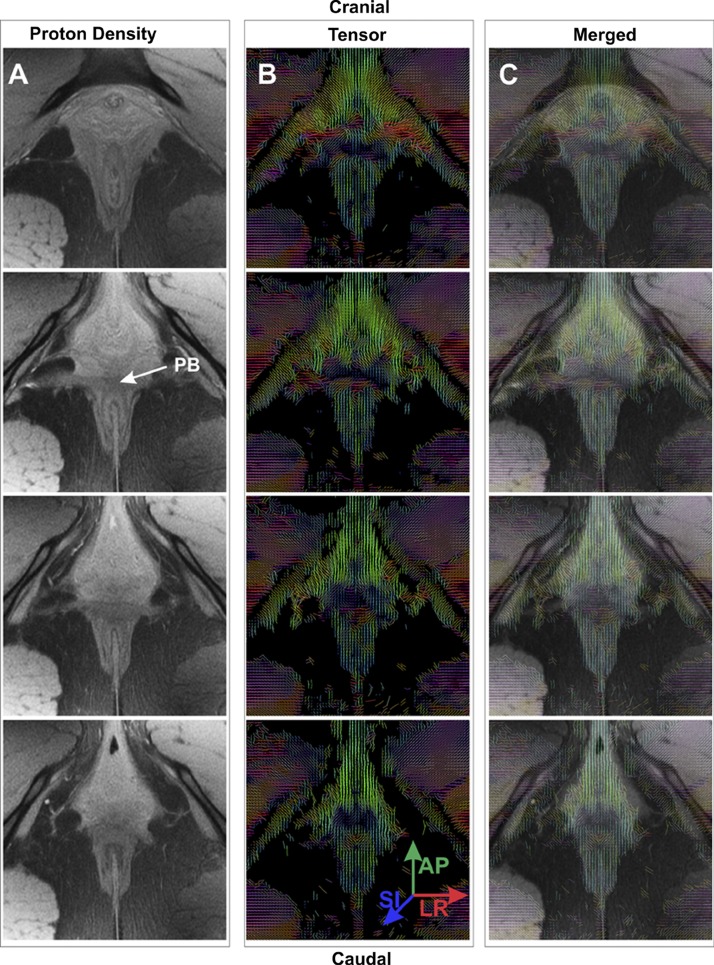
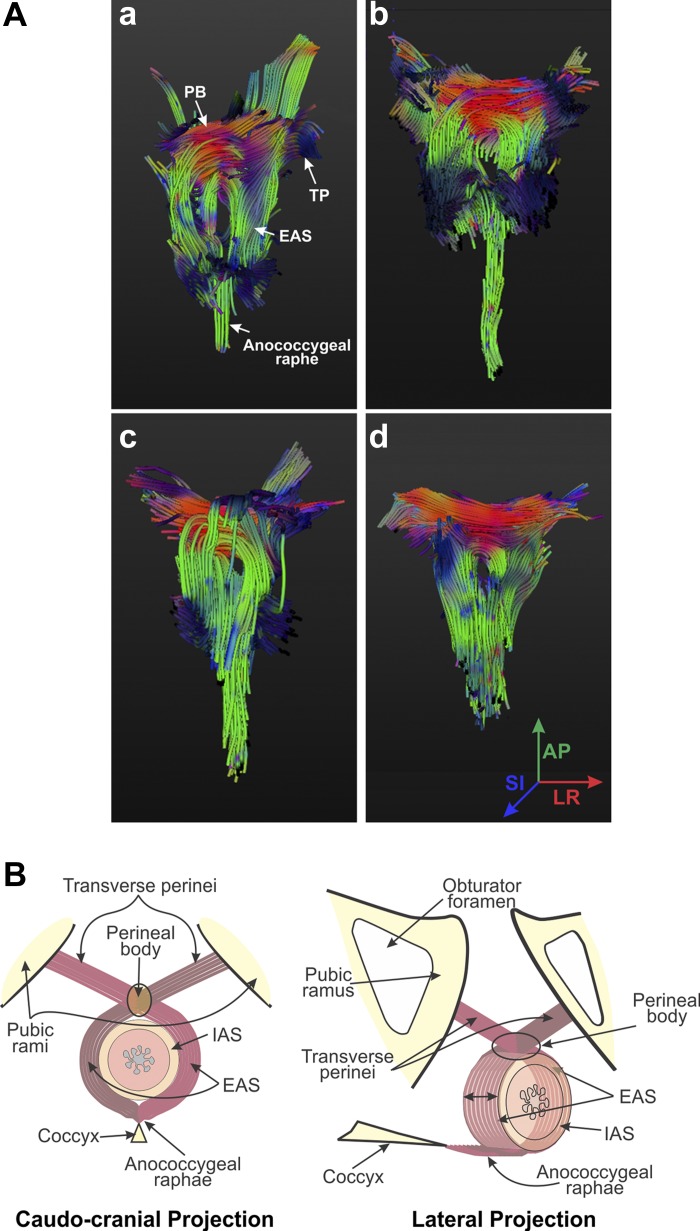
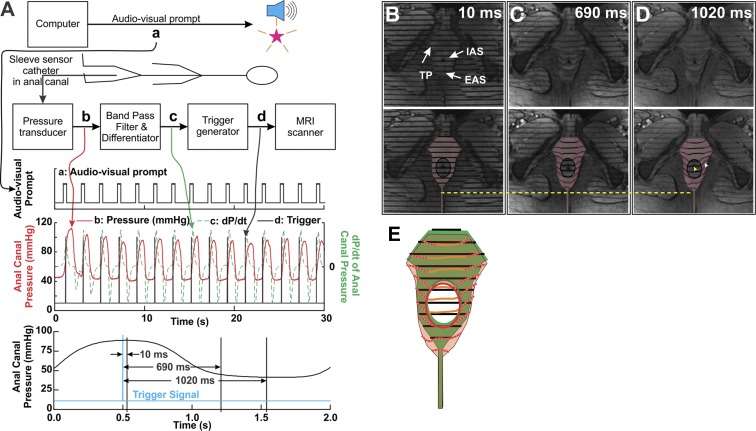
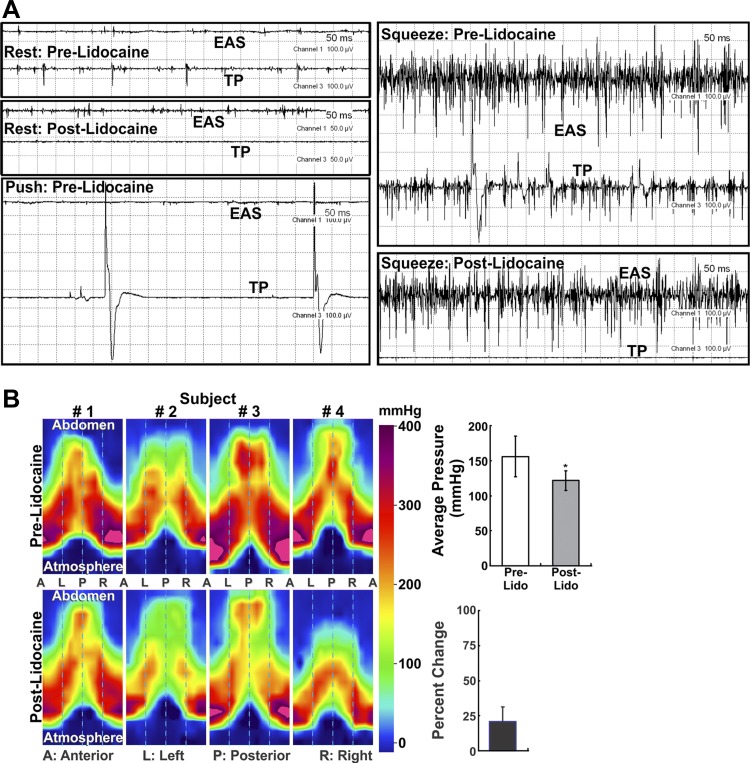
The external anal sphincter (EAS) may be injured in 25-35% of women during the first and subsequent vaginal childbirths and is likely the most common cause of anal incontinence. Since its first description almost 300 years ago, the EAS was believed to be a circular or a "donut-shaped" structure. Using three-dimensional transperineal ultrasound imaging, MRI, diffusion tensor imaging, and muscle fiber tracking, we delineated various components of the EAS and their muscle fiber directions. These novel imaging techniques suggest "purse-string" morphology, with "EAS muscles" crossing contralaterally in the perineal body to the contralateral transverse perineal (TP) and bulbospongiosus (BS) muscles, thus attaching the EAS to the pubic rami. Spin-tag MRI demonstrated purse-string action of the EAS muscle. Electromyography of TP/BS and EAS muscles revealed their simultaneous contraction and relaxation. Lidocaine injection into the TP/BS muscle significantly reduced anal canal pressure. These studies support purse-string morphology of the EAS to constrict/close the anal canal opening. Our findings have implications for the effect of episiotomy on anal closure function and the currently used surgical technique (overlapping sphincteroplasty) for EAS reconstructive surgery to treat anal incontinence.
Keywords: anal incontinence; childbirth-related injury; external anal sphincter muscle architecture; magnetic resonance diffusion tensor imaging.
Figures
Similar articles
-
Functional morphology of anal sphincter complex unveiled by high definition anal manometery and three dimensional ultrasound imaging.Neurogastroenterol Motil. 2011 Nov;23(11):1013-9, e460. doi: 10.1111/j.1365-2982.2011.01782.x. Epub 2011 Sep 25. Neurogastroenterol Motil. 2011. PMID: 21951657 Free PMC article.
-
Usefulness of anorectal and endovaginal 3D ultrasound in the evaluation of sphincter and pubovisceral muscle defects using a new scoring system in women with fecal incontinence after vaginal delivery.Int J Colorectal Dis. 2017 Apr;32(4):499-507. doi: 10.1007/s00384-016-2750-z. Epub 2016 Dec 29. Int J Colorectal Dis. 2017. PMID: 28035460
-
Anal sphincter defects and fecal incontinence 15-24 years after first delivery: a cross-sectional study.Ultrasound Obstet Gynecol. 2018 May;51(5):677-683. doi: 10.1002/uog.18827. Ultrasound Obstet Gynecol. 2018. PMID: 28782264
-
Anorectal Anatomy and Function.Gastroenterol Clin North Am. 2022 Mar;51(1):1-23. doi: 10.1016/j.gtc.2021.10.001. Gastroenterol Clin North Am. 2022. PMID: 35135656 Review.
-
Perineal scar endometriosis involving the anal sphincter. A case report and review of the literature.Ann Ital Chir. 2021 Jan 20;10:S2239253X2103173X. Ann Ital Chir. 2021. PMID: 33480866 Review.
Cited by
-
High-frequency ultrasound imaging of the anal sphincter muscles in normal subjects and patients with fecal incontinence.Neurogastroenterol Motil. 2019 Apr;31(4):e13537. doi: 10.1111/nmo.13537. Epub 2019 Jan 24. Neurogastroenterol Motil. 2019. PMID: 30680849 Free PMC article.
-
Understanding the physiology of human defaecation and disorders of continence and evacuation.Nat Rev Gastroenterol Hepatol. 2021 Nov;18(11):751-769. doi: 10.1038/s41575-021-00487-5. Epub 2021 Aug 9. Nat Rev Gastroenterol Hepatol. 2021. PMID: 34373626 Review.
-
Loop analysis of the anal sphincter complex in fecal incontinent patients using functional luminal imaging probe.Am J Physiol Gastrointest Liver Physiol. 2020 Jan 1;318(1):G66-G76. doi: 10.1152/ajpgi.00164.2019. Epub 2019 Nov 18. Am J Physiol Gastrointest Liver Physiol. 2020. PMID: 31736339 Free PMC article.
-
Evaluation of Age- and Radical-Prostatectomy Related Changes in Male Pelvic Floor Anatomy Based on Magnetic Resonance Imaging and 3-Dimensional Reconstruction.World J Mens Health. 2021 Jul;39(3):566-575. doi: 10.5534/wjmh.200021. Epub 2020 Jun 1. World J Mens Health. 2021. PMID: 32648374 Free PMC article.
-
Contrast-enhanced Micro-CT imaging of a foetal female pelvic floor reveals anatomical details.PLoS One. 2025 Jun 13;20(6):e0314261. doi: 10.1371/journal.pone.0314261. eCollection 2025. PLoS One. 2025. PMID: 40512734 Free PMC article.
References
-
- Arakawa T, Hayashi S, Kinugasa Y, Murakami G, Fujimiya M. Development of the external anal sphincter with special reference to intergender difference: observations of mid-term fetuses (15–30 wk of gestation). Okajimas Folia Anat Jpn 87: 49–58, 2010. - PubMed
-
- Bharucha AE. Pelvic floor: anatomy and function. Neurogastroenterol Motil 18: 507–519, 2006. - PubMed
-
- Bo K, Lilleas F, Talseth T, Hedland H. Dynamic MRI of the pelvic floor muscles in an upright sitting position. Neurourol Urodyn 20: 167–174, 2001. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources