

Hospitalizations following living donor nephrectomy in the United States
- PMID: 24458071
- PMCID: PMC3913232
- DOI: 10.2215/CJN.03820413
Hospitalizations following living donor nephrectomy in the United States
Abstract
Background and objectives: Living donors represented 43% of United States kidney donors in 2012. Although research suggests minimal long-term consequences of donation, few comprehensive longitudinal studies for this population have been performed. The primary aims of this study were to examine the incidence, risk factors, and causes of rehospitalization following donation.
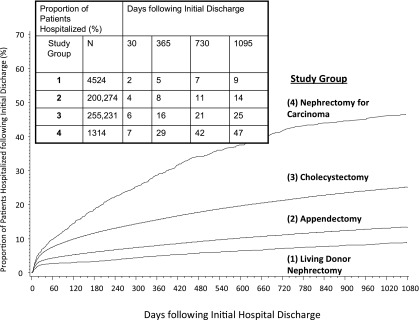
Design, setting, participants, & measurements: State Inpatient Databases (SID) compiled by the Agency for Healthcare Research and Quality were used to identify living donors in four different states between 2005 and 2010 (n=4524). Multivariable survival models were used to examine risks for rehospitalization, and patient characteristics were compared with data from the Scientific Registry of Transplant Recipients (SRTR). Outcomes among patients undergoing appendectomy (n=200,274), cholecystectomy (n=255,231), and nephrectomy for nonmetastatic carcinoma (n=1314) were contrasted.
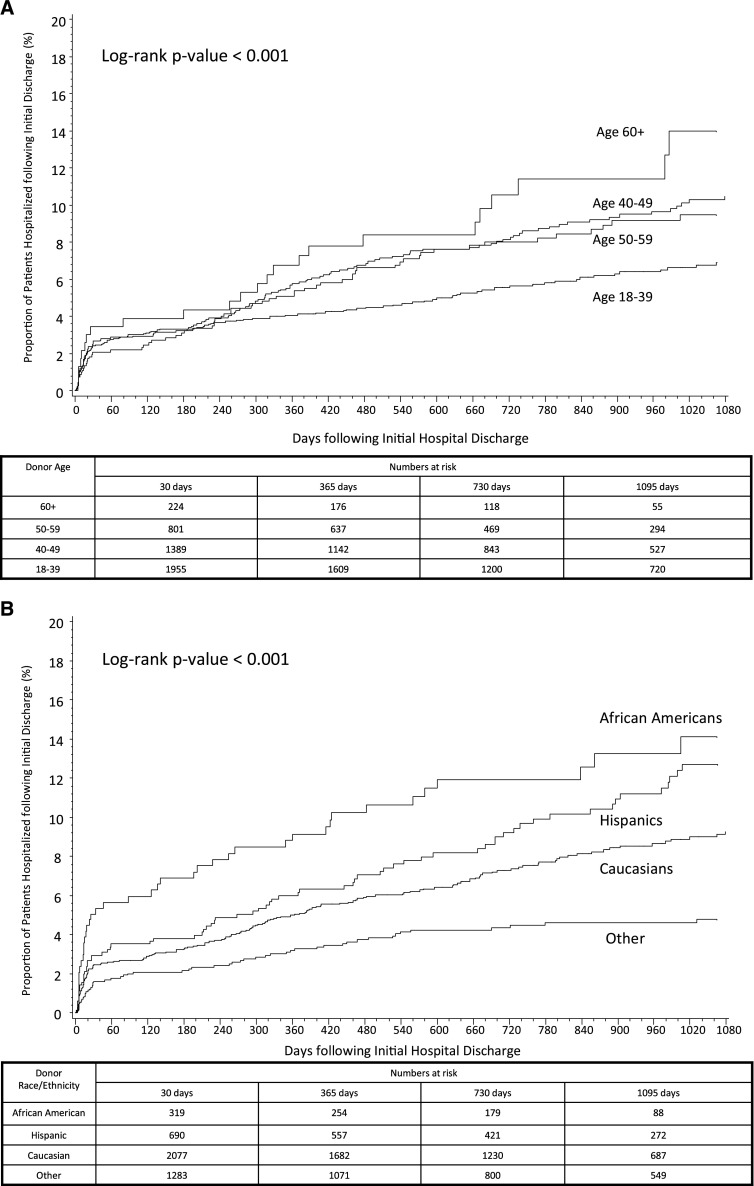
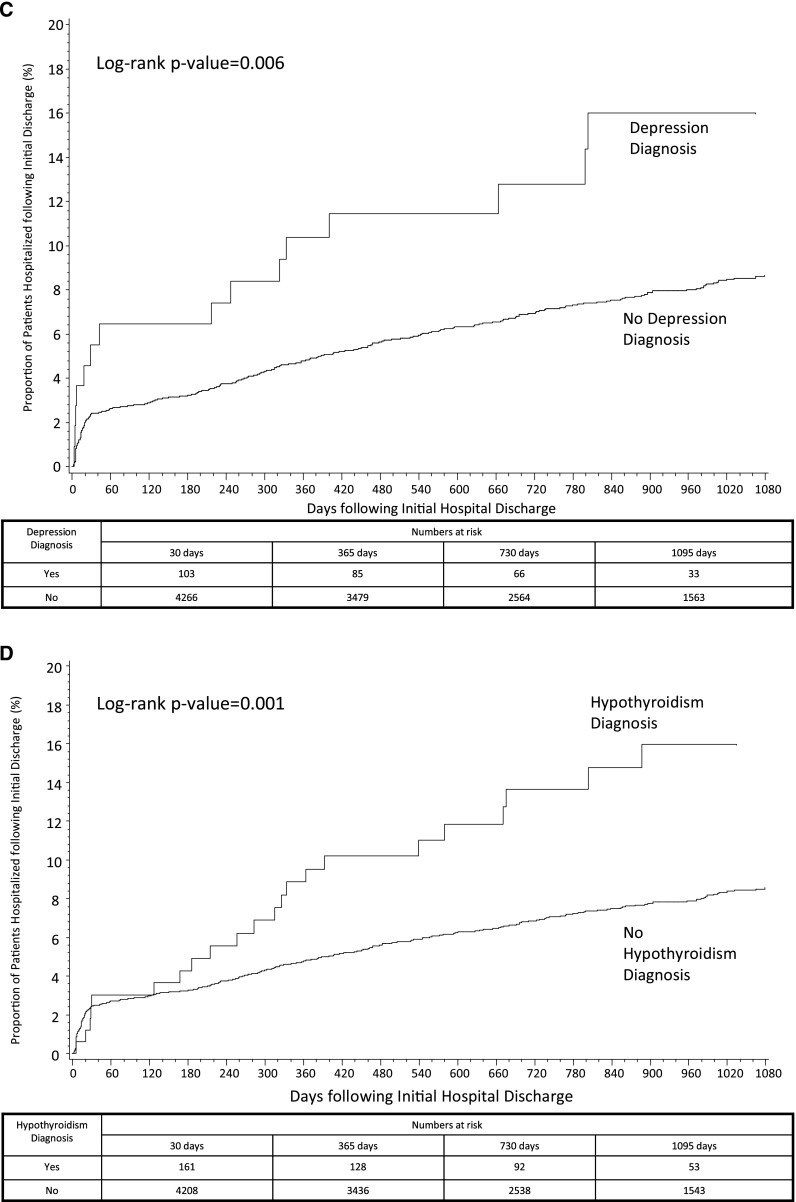
Results: The study population was similar to United States donors (for SRTR and SID, respectively: mean age, 41 and 41 years; African Americans, 12% and 10%; women, 60% and 61%). The 3-year incidence of rehospitalization following donation was 11% for all causes and 9% excluding pregnancy-related hospitalizations. After censoring of models for pregnancy-related rehospitalizations, older age (adjusted hazard ratio [AHR], 1.02 per year; 95% confidence interval [95% CI], 1.01 to 1.03), African American race (AHR, 2.16; 95% CI, 1.54 to 3.03), depression (AHR, 1.88; 95% CI, 1.12 to 3.14), hypothyroidism (AHR, 1.63; 95% CI, 1.06 to 2.49), and longer initial length of stay were related to higher rehospitalization rates among donors. Compared with living donors, adjusted risks for rehospitalizations were greater among patients undergoing appendectomy (AHR, 1.58; 95% CI, 1.42 to 1.75), cholecystectomy (AHR, 2.25; 95% CI, 2.03 to 2.50), and nephrectomy for nonmetastatic carcinoma (AHR, 2.95; 95% CI, 2.58 to 3.37). Risks for rehospitalizations were higher among African Americans than whites in each of the surgical groups.
Conclusions: The SID is a valuable source for evaluating characteristics and outcomes of living kidney donors that are not available in traditional transplant databases. Rehospitalizations following donor nephrectomy are less than seen with other comparable surgical procedures but are relatively higher among donors who are older, are African American, and have select comorbid conditions. The increased risks for rehospitalizations among African Americans are not unique to living donation.
Figures
Comment in
-
Rehospitalization after living kidney donation.Clin J Am Soc Nephrol. 2014 Feb;9(2):227-8. doi: 10.2215/CJN.12701213. Epub 2014 Jan 23. Clin J Am Soc Nephrol. 2014. PMID: 24458083 Free PMC article. No abstract available.
References
-
- Organ Procurement and Transplantation Network. Donors recovered in the U.S. by donor type. Available at: http://optn.transplant.hrsa.gov/data/ August 14, 2013.
-
- Gill JS, Schaeffner E, Chadban S, Dong J, Rose C, Johnston O, Gill J: Quantification of the early risk of death in elderly kidney transplant recipients. Am J Transplant 13: 427–432, 2013 - PubMed
-
- Segev DL, Muzaale AD, Caffo BS, Mehta SH, Singer AL, Taranto SE, McBride MA, Montgomery RA: Perioperative mortality and long-term survival following live kidney donation. JAMA 303: 959–966, 2010 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
